hypertension
27th Annual Meeting and Exposition of the American Society of Hypertension (ASH)
Latest Hypertension Updates Further Determine Ideal Blood Pressure Targets and Treatment
New York – Many presentations at the recent 27th Annual Meeting and Exposition of the American Society of Hypertension (ASH) focused on core hypertension-related questions: Which agents are best? What are the best combinations? What are the ideal target blood pressure levels? Interest in research pursuing these questions remains strong given that hypertension, one of the most common conditions among middle-aged and older adults, is a leading risk factor for stroke, heart disease and cardiac events, chronic kidney disease, and other ailments.
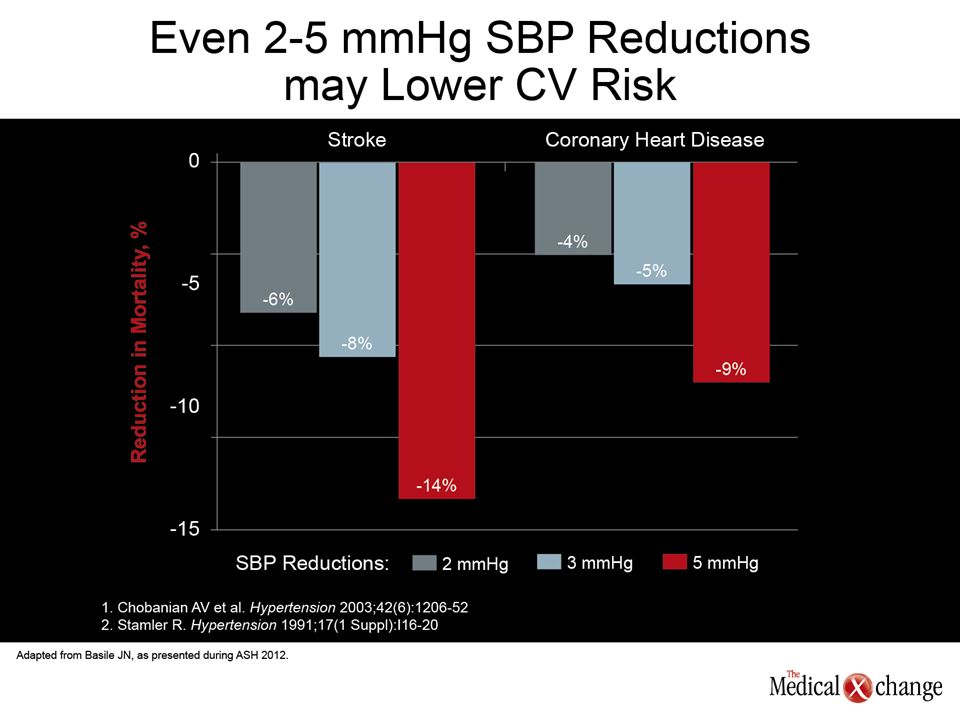
Dr. Jan N. Basile, Professor of Medicine, Medical University of South Carolina, noted that approximately 68 million adults in the United States, 31% of the population, are hypertensive. In addition, the risk of cardiovascular (CV) death is estimated to double with each 20/10 mmHg increase in blood pressure (BP) (Chobanian AV et al. JAMA 2003;289(19):2560-72; Lewington S et al. Lancet 2002;360(9349):1903-1913). Importantly, even modest reductions in systolic blood pressure (SBP) can have substantial risk-lowering effects (Fig. 1). While that fact is encouraging, Dr. Basile underscored that as many as 50% of patients with hypertension are not adequately controlled.
Combination Therapy for Lower SBP Goal
As presented at this year’s ASH meeting, Dr. Karen C. Johnson, The University of Tennessee Health Science Center, Memphis, reviewed data (Bakris GL et al. Am J Kidney Dis. 2000;36(3):646-61) showing that in nine major clinical trials of antihypertensive medications, a mean of about three agents was required to achieve systolic targets for BP. She further noted that targeting an intensive lower goal of <120 mmHg in the Action to Control CV Risk in Diabetes (ACCORD) trial failed to reduce the primary endpoint of CV disease events compared with the standard target of <140 mmHg among 4,700 type 2 diabetes patients. Stroke was reduced, but at the cost of increased side effects in the intensive target group (ACCORD Study Group et al. N Engl J Med. 2010;362(17):1575-85). Dr. Johnson described The Systolic Blood Pressure Intervention Trial (SPRINT), currently about 60% enrolled, which will test the hypothesis that benefits for treating individuals at high risk for CV disease to a lower SBP goal will outweigh the risks.
Dr. Basile presented data from trials on a fixed-dose combination of azilsartan medoxomil (AZL-M), a new and recently approved angiotensin receptor blocker (ARB), and chlorthalidone (CLD), a thiazide-like diuretic. After 8 weeks of treatment with a 40 mg AZL-M/25 mg CLD combination, clinic systolic/diastolic reductions were 39.5/17.0 mmHg in a cohort of 1714 patients with baseline systolic clinic pressures of ≥160 mmHg and ≤190 mmHg.
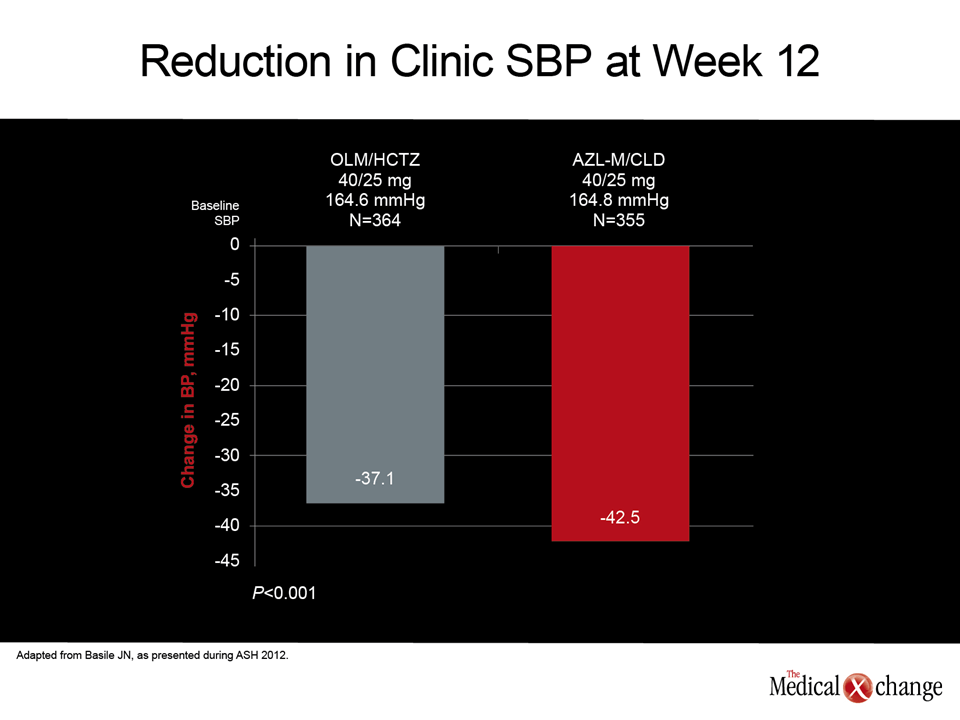
Also, a comparison of fixed-dose AZL-M/CLD with olmesartan (OLM)/hydrochlorothiazide (HCTZ) among 719 patients revealed a statistically significant benefit for those receiving AZL-M/CLD (P<0.001), with a 42.5 mmHg systolic reduction vs. 37.1 mmHg for the OLM/HCTZ combination (Fig. 2).
The benefit was consistent across all subpopulations. Significantly more AZL-M/CLD patients achieved the <140/<90 mmHg target (81.4% versus 74.6% for OLM/HCTZ, P=0.021). Among adverse events reported at higher incidence for AZL-M/CLD than for the OLM/HCTZ combination, only fatigue (2.0%) and dizziness (8.9%) occurred at rates of 2.0% or higher.
Determining the Second Agent in Fixed-dose Combination Therapy
Commenting in an interview on the choice of CLD or HCTZ as the second agent in a fixed-dose combination, Dr. Basile noted that while there have been no head-to-head comparison trials of HCTZ versus CLD, the best outcomes for HCTZ were reported in trials 40 years ago when HCTZ was given at much higher doses (50-100 mg) than currently. Clinicians have since opted for HCTZ doses of 12.5-25 mg because of hypokalemia, hyperglycemia and tolerability issues at higher doses. “It’s hard to find well-designed trials showing benefit for the currently-prescribed lower doses of HCTZ versus placebo or other comparators,” Dr. Basile said. Comparisons of CLD at 12.5 to 25 mg to placebo in Systolic Hypertension in the Elderly Program (SHEP), Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) and some other trials, he added, do show significant benefit. Given those data and longer half-life of CLD, Dr. Basile added, “makes CLD a better BP-lowering agent at present doses.” In a separate ASH session on JNC-8, JNC-8 panelists Drs. Barry Carter, William Cushman, and Suzanne Oparil all advocated for CLD as the preferred diuretic for the treatment of hypertension based on its superior BP-lowering characteristics and longer half-life.
Difficult-to-Treat Populations
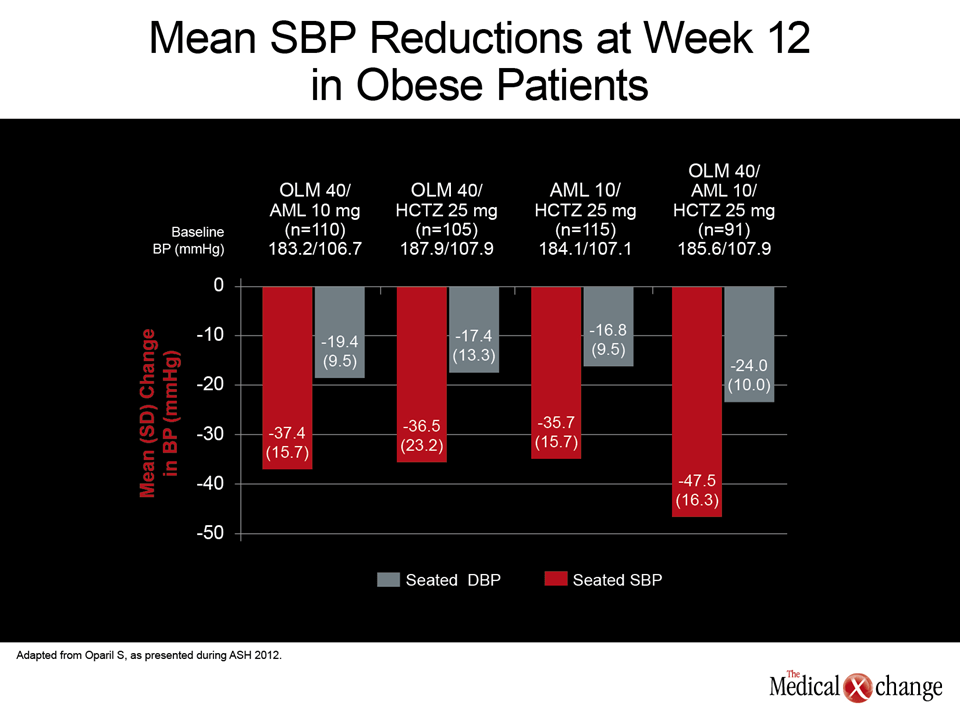
As presented at ASH by Dr. Suzanne Oparil, Professor of Medicine, University of Alabama, Birmingham of the Triple Therapy with Olmesartan Medoxomil, Amlodipine, and Hydrochlorothiazide in Hypertensive Patients Study (TRINITY), data compared triple antihypertensive therapy versus dual therapy in obese and non-obese patients, many with severe hypertension. Triple therapy in 600 patients consisted of OLM (40 mg), amlodipine (AML) (10 mg) and HCTZ (25 mg), and dual therapy consisted of two-agent permutations of the three agents (at the same doses).
For patients receiving dual therapies, SBP reductions ranged from 27.4 mmHg (OLM/AML) to 31.2 mmHg (OLM/HCTZ) in obese subjects and from 30.5 mmHg (OLM/HCTZ) to 34.0 mmHg (OLM/AML) in non-obese subjects. For triple therapy the reductions were 37.9 and 39.1 mmHg in obese and non-obese subjects, respectively.
BP reductions were more substantial among those with severe hypertension; SBP reductions were 47.5 and 47.4 mmHg in obese and non-obese subjects, respectively (Fig. 3). Dual therapy reductions in this subset were ~11 mmHg smaller (35.7 to 37.4 mmHg) among obese subjects and ~9 mmHg smaller (38.6 to 39.3 mmHg) among non-obese subjects.
“This finding from the TRINITY trial is important,” stated Dr. Oparil, “because a third of Americans are obese, and it is known that it is more difficult to bring BP down by any given amount in obese subjects.”
Conclusion
For the treatment of hypertensive patients, it has been shown that even modest reductions in SBP can have substantial risk-lowering effects. Studies presented at this year’s ASH meeting advocated the use of fixed-dose combinations as first therapy to help patients reach target.