Expert Review
13th European AIDS Clinical Society (EACS) Conference: Expert Review
Protease Inhibitors in Nucs-Sparing Strategies: Report from the EACS
Dr. Patrice Junod
Clinique Médicale l’Actuel, Montreal, QC
Dr. M. John Gill
Southern Alberta HIV Clinic, Calgary, AB
Belgrade – Antiretroviral combinations that do not include nucleoside reverse transcriptase inhibitors (NRTIs; ‘nucs’), so-called nucs-sparing regimens, were once largely tested as a strategy to avoid mitochondrial toxicities. However, this approach now offers promise in reducing some of the specific age-related morbidities exacerbated by NRTIs, such as progressive renal impairment. It could also save costs. At the 13th European AIDS Clinical Society (EACS) meeting, a variety of new information was presented on the role of protease inhibitors (PIs) in nucs-sparing regimens. Whether combined with another PI or a drug from another class, such regimens were reported as already being in routine use at some centres even while clinical studies attempt to define which patients are the best candidates. Overall, the data presented suggested that nucs-sparing is a reasonable and appropriate option in at least some select patient groups for whom NRTIs are relatively contraindicated. As more data become available, this approach may beextended to the larger HIV population, including those who are treatment naive.
Protease Inhibitors in Nucs-Sparing Therapy
The addition of protease inhibitors (PIs) to a double nucleoside backbone was a landmark event in the HIV epidemic as it permitted sustained control of human immunodeficiency virus (HIV) infection. Fifteen years later, these drugs remain an important option in HIV treatment, but their role continues to evolve. While PIs are no longer essential for effective first-line therapy in all treatment-naive patients, they continue to exhibit versatility in a broad spectrum of indications, including treatment regimens designed to address high viral loads or low CD4+ cell counts. The classic combination of a PI with two nucleoside reverse transcriptase inhibitors (NRTIs) remains viable and useful, but data presented at the 13th European AIDS Clinical Society (EACS) meeting documented increasing attention to the potential role of PIs for nucs-sparing. This approach can simplify treatment but was also tested for its role in improving tolerability and safety.
While nucs-sparing strategies have been and are still applied on an individual basis, new and larger studies testing this approach suggest it may have a far wider potential for clinical use.
Nucs-sparing antiretroviral therapy is not a new concept. Interest in this approach was initially driven by its potential to reduce or avoid mitochondrial toxicity. Antiretroviral-associated mitochondrial toxicity, which can manifest in a variety of ways, including lactic acidosis, myopathy, and changes in body fat distribution, was identified more than a decade ago and soon after the introduction of triple-drug combinations. The thymidine analogue NRTIs were widely considered the cause of mitochondrial toxicity as these agents bind to a variety of host polymerases as well as the viral reverse transcriptase. One of these, the gamma DNA polymerase, is responsible for replication of mitochondrial DNA. Nucs-sparing strategies, which do reduce risk of mitochondrial toxicity, have been and are still applied on an individual basis, but new and larger studies testing this approach suggest it may have a far wider potential for clinical use.
New Data from PROGRESS Study
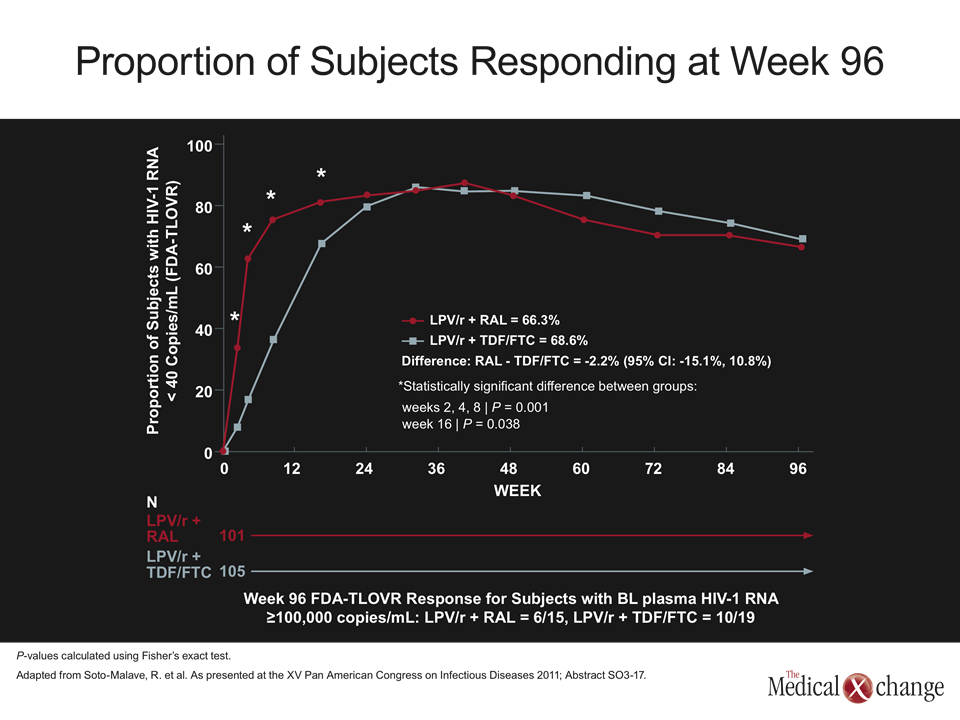
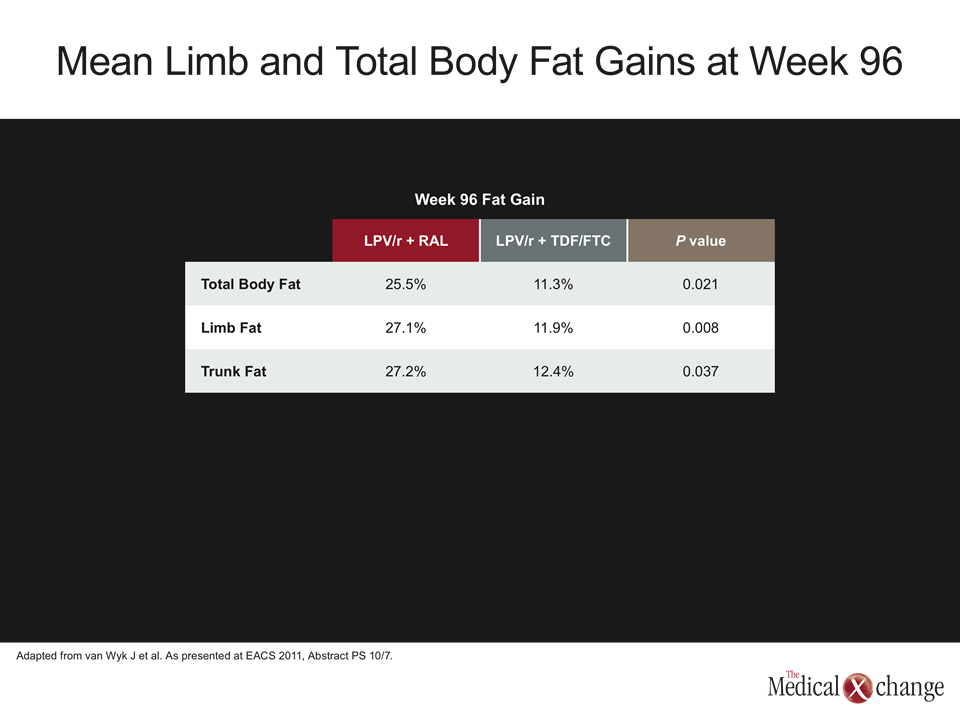
Of recent or emerging data on nucs-sparing strategies, the results of the PROGRESS trial are among the most significant. Initial 48-week data were presented at the 2010 International AIDS Society (IAS) meeting in Vienna (Reynes J et al. As presented at IAS 2010; Abstract MOAB0101). More recently, 96-week data were presented at the XV Pan American Congress on Infectious Diseases in Punta del Este, Uruguay. In PROGRESS, 206 antiretroviral naïve patients were randomized to either a two-drug regimen containing ritonavir-boosted lopinavir (LPV/r) and the integrase inhibitor raltegravir (RAL) or to a three-drug regimen containing LPV/r plus the NRTIs tenofovir and emtricitabine (TDF/FTC). The nucs-sparing combination, which provided almost identical viral suppression through 96 weeks of follow-up, was found non-inferior (Fig. 1). In the new data from PROGRESS presented at the EACS, the treatment regimens were compared for body fat distribution changes after 96 weeks of therapy (van Wyk J et al. Abstract PS 10/7). In this substudy of PROGRESS, full-body dual-energy X-ray absorptiometry (DXA) scans were conducted at baseline and weeks 48 and 96. The radiologist interpreting the scans was blinded to the treatment assignment. While total body fat, limb fat, and trunk fat were increased over 96 weeks on both regimens, the mean limb and total body fat gains were significantly greater in the LPV/r plus RAL group, according to data presented by Dr. Pere Domingo, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain. Specifically, the gains at 96 weeks in total body fat (25.5% vs. 11.3%; P=0.021), total limb fat (27.1% vs. 11.9%; P=0.008) and total trunk fat (27.2% vs. 12.4%; P=0.037) were more than twice as great in the group receiving the nucs-sparing regimen (Table 1). The percentages of patients with exceptionally high fat loss, such as >20% or >30%, or those with exceptionally high trunk fat gain, such as >20% or >30%, were similar in the two groups. Body mass index (BMI) did not affect relative differences in limb fat gain between regimens, but patients with a low baseline BMI gained more fat over the course of therapy. Several factors independent of therapy were associated with a >20% fat loss over the course of the study, including evidence of elevated insulin resistance (P=0.023), a baseline CD4+ count <200 cell/mm3 (P=0.019), non-White race (P=0.008), and elevated inflammatory activity as indicated by elevated serum levels of tumor necrosis factor (TNF). These body fat distribution findings provide support for the basic premise that nucs-sparing may have metabolic advantages over the conventional combination of a PI and two NRTIs. Although mitochondrial toxicity was not specifically evaluated in this analysis, the relative disadvantage for body fat gain in the arm receiving the NRTI combination of TDF/FTC is consistent with this mechanism of action.
HIVNAT019: Two-PI Nucs-Sparing Results
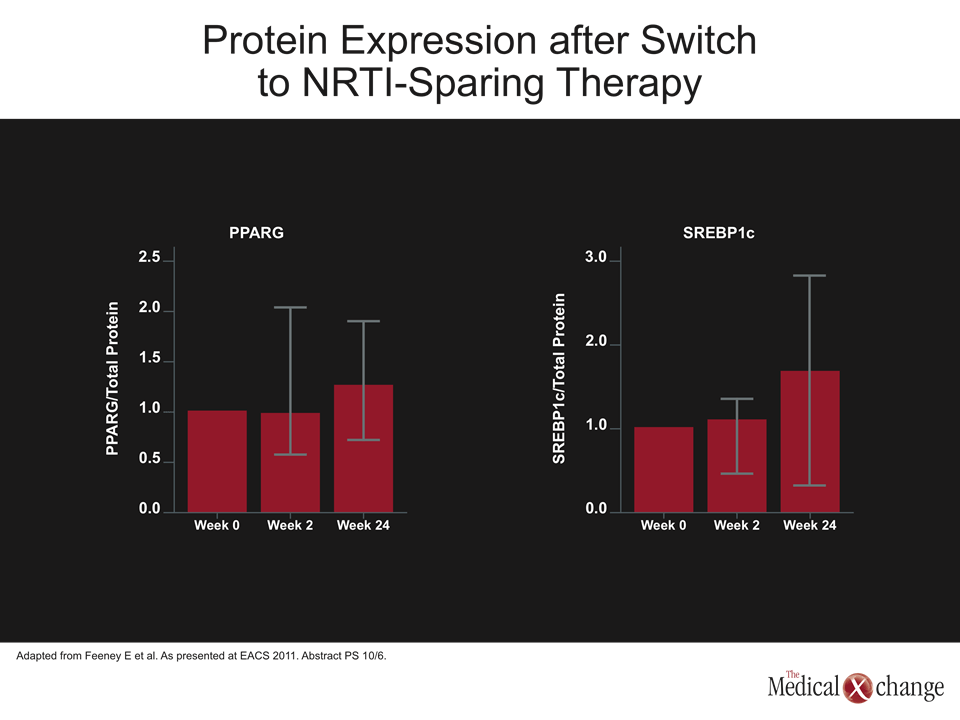
Further support for this premise was provided by the separate HIVNAT019 study, which performed sophisticated analysis of subcutaneous adipose tissue mitochondrial function studies in patients receiving a nucs-sparing regimen of LPV/r plus saquinavir (SQV) (Feeney E et al. Abstract PS 10/6). In the study, presented at EACS 2011 by Dr. Eoin R. Feeney, HIV Molecular Research Group, School of Medicine and Medical Sciences, University College, Dublin, Ireland, flank subcutaneous adipose tissue biopsies were taken at baseline and at weeks 2 and 24 in 20 treatment-naive patients on the dual PI regimen. An analysis was then performed on protein content and gene expression in the mitochondrial DNA. At week 24, dual PI therapy showed increases from baseline in both SREBP1c and PPARG, which are associated with upregulation of adipogenesis. This double PI regimen was also associated with a reduction in nuclear-derived mitochondrial protein. While this study suggests that HIV patients have already developed at least some degree of mitochondrial dysfunction prior to the initiation of antiretroviral therapy based on the improvements in SREBP1c and PPARG, it also suggests that a six-month nucs-sparing therapy can reverse these effects.
New Data from MONARCH at the EACS: PI Monotherapy
The MONARCH study, which compared ritonavir-boosted darunavir (DRV/r) monotherapy to a conventional DRV/r plus two NRTIs regimen, also generated new data suggesting that nucs-sparing regimens can favourably affect body fat redistribution data (Guaraldi G et al. Abstract PE7.5/4). In this relatively small but prospective study of 30 patients, bone mineral density (BMD), visceral adipose tissue, and leg fat were assessed over the course of the study. While there were no virologic failures in either group after 48 weeks of therapy, changes in BMD and fat distribution were seen from baseline in both groups. Visceral adipose fat loss was similar between the two groups, but leg fat loss was substantially greater in the group receiving NRTIs. There was no bone loss in the lumbar or femoral sites in the NRTI arm, but there was a slight gain in the nucs-sparing arm. The authors of the study, although cautioning that data are preliminary, reported that a nucs-sparing DRV/r monotherapy appears to improve BMD and fat distribution. In addition to these data, broader use of simplified nucs-sparing regimens is also being encouraged as a standard of care by some centres which are systematically reviewing and reporting on their experiences. In a multicentre retrospective review of 110 such patients treated in Spain, the estimated probability of remaining on a nucs-sparing therapy with DRV/r was 88% in newly-presented data (Perez-Elias MJ et al. Abstract PE7.5/3). In this series, which evaluated DRV/r monotherapy, most of the patients had switched to this PI monotherapy regimen to avoid NRTI toxicity. At week 48, viral control was maintained with DRV/r monotherapy in 82% on an ITT analysis and 90.2% in the on-treatment analysis. According to the data, presented by Dr. Maria J. Perez-Elias, Hospital Ramon y Cajal, Madrid, Spain, the therapy was well tolerated, and there were no AIDS-defining events. A univariate and multivariate analysis did not identify any factors that predicted response.
Nucs-sparing regimens do appear to be reasonable in carefully selected patients with NRTI-related adverse events.
In another set of data generated within the same study, tolerability was assessed in the 66 (60%) of the 110 patients who had switched to DRV/r monotherapy because of toxicity experienced on their previous regimen (Martinez-Colubi M et al. Abstract PE7.9/12). In the 41 evaluable patients, toxicity was reduced in 34 (81%). This included 100% of those who previously reported liver toxicity, bone toxicity, or gastrointestinal toxicity, 78% of those with previously reported renal toxicity, 67% of those with dyslipidemia, and 57% of those with lipodystrophy. Based on the fact that good viral suppression was maintained, the authors of this study suggested that nucs-sparing regimens do appear to be reasonable in carefully selected patients with NRTI-related adverse events.
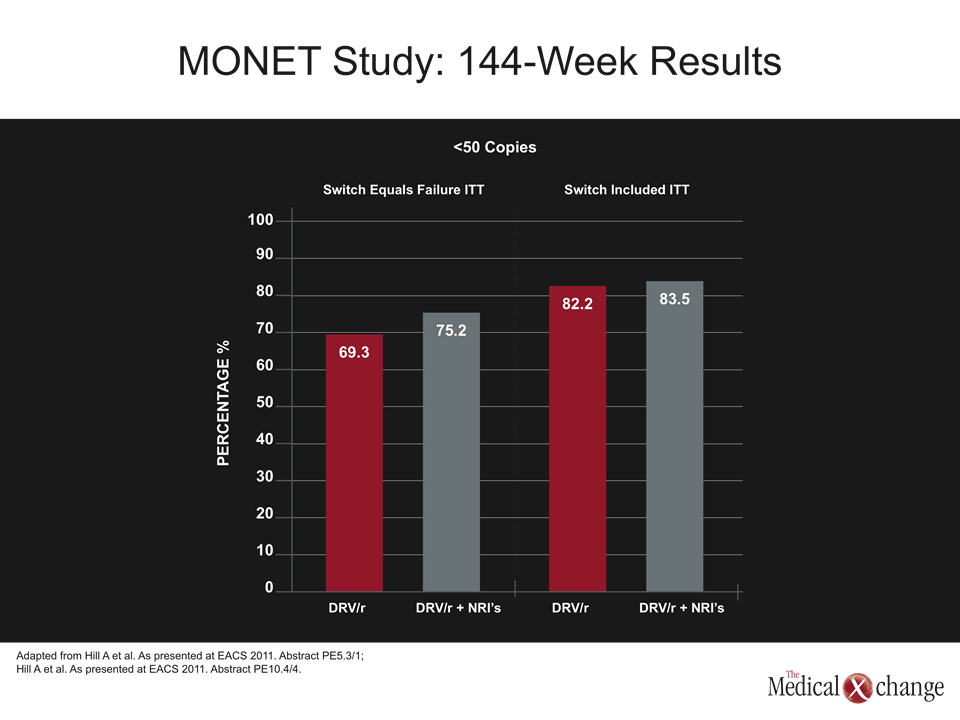
MONET Data at 144 Weeks: PI Monotherapy
The MONET trial compared a switch to DRV/r monotherapy with DRV/r and two NRTIs in patients already on therapy with viral load suppression (<50 HIV RNA copies/mL). A new analysis looked at both resistance and cost of care. In the final 144-week data, presented by Dr. Federico Pulido, Hospital 12 de Octubre, Madrid, Spain, the switch-included ITT analysis showed similar efficacy for DRV/r (82.2%) relative to DRV/r plus NRTIs (83.5%) (Hill A et al. Abstract PE5.3/1). Dr. Pulido reported that there has been no overall evolution of new minor PI mutations documented in either treatment arm in repeated genotyping, supporting the premise that this regimen is viable in selected patients. Hepatitis C virus (HCV) co infected patients, however, did far worse on monotherapy. At 96 weeks, only 43.5% of those with HCV co-infection remained optimally suppressed (<50 copies/mL) versus 73.3% of those who did not have co-infection. Despite this limitation, a separate MONET analysis concluded that large cost savings would be realized by patients who switch to DRV/r monotherapy from more complicated regimens (Gazzard A et al. Abstract PE10.4/4). As calculated using UK costs, the savings of more than $200 million over three years were derived from the lower overall drug costs. Nucs-sparing has been largely pursued to avoid toxicities, but treatment simplification remains an important goal in treatment-experienced patients. While simplification is of limited relevance in first-line regimens that only require one or two pills daily, treatment-experienced patients sometimes acquire new agents without eliminating NRTIs that are already in the regimen. In a study from Montreal, a simplification strategy built on removing non-active NRTIs from the regimen was tested for efficacy (Trottier B et al. Abstract PE7.5/1). In this prospective study of 31 patients with a mean age of 50 years, a mean time on treatment of 14 years, and well controlled HIV, patients were followed after non-active NRTIs as determined by genotypic studies were removed from the regimen.
The average reduction in annual cost by eliminating non-effective NRTIs was more than 10%.
After 24 weeks of treatment simplification, 100% of the patients remained with an undetectable viral load while gaining 10 CD4+ cells/mm3. Although the gain in CD4+ cells was not significant, there were numerous advantages, including a mean annual reduction in cost of >$3000 (Canadian). There were no new laboratory abnormalities of grade 2 or greater or any other serious adverse events. The most commonly discontinued NRTIs were lamivudine (3TC) and FTC. The authors of the study, led by Dr. Benoit Trottier, Clinique Medical L’Actuel, Montreal, Quebec, estimated that the average reduction in annual cost by eliminating non-effective NRTIs was more than 10%.
Nucs-sparing to Reduce Age-related Morbidities
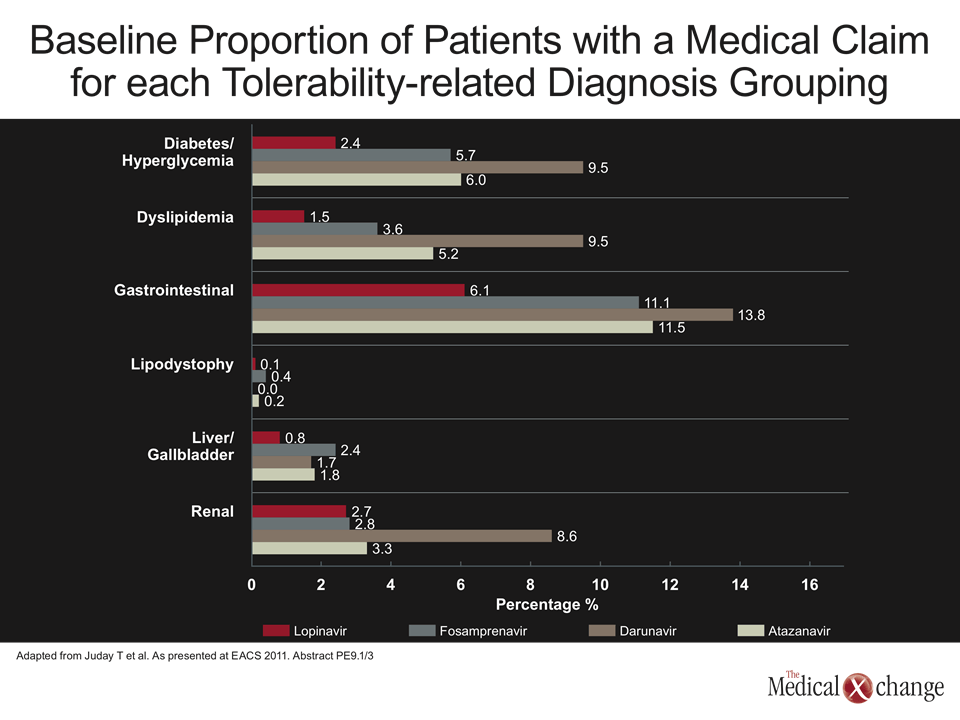
The role of nucs-sparing for avoiding the accelerated age-related non-infectious co-morbidities of HIV infection have been less well explored, but increasing attention toward these strategies is expected. Typical of many recent studies, new data on the causes of death in the era of effective anti-retroviral therapy emphasize that diseases of aging, such as cardiovascular disease (CVD) and malignancy, may soon supersede AIDS as major cause of death in HIV-infected populations (Klötgen H-W et al. As presented at EACS 2011. Abstract PE18.4/8). In a retrospective chart review of patients managed at a university hospital in Essen, Germany, causes of death were compared in three periods: 01/1998-10/2003, 11/2003-08/2007, and 09/2007-12/2009. Death due to AIDS-defining illnesses fell from 36% in the earliest period to 22% in the latest period. In the most recent period, all of the AIDS deaths were associated with late presenting cases. Over the course of the same three periods, death due to myocardial infarction (MI) climbed from 0% to 7% while death due to malignancy climbed from 9% to 24%. In general, it has been estimated that age-related morbidities, such as CVD, BMD loss, renal impairment, and cognitive dysfunction, may occur 10 to 15 years earlier in patients with HIV when compared to individuals without HIV. Various hypotheses for this accelerated morbidity have been proposed, of which an upregulated inflammatory state is among the most prominent. Importantly, it is reasonable to expect that nucs-sparing regimens would be effective in reducing NRTI-related side effects that contribute to age-related diseases. For example, the renal toxicity associated with TDF may be relevant to a potential for increased risk of both CVD and osteoporosis, both of which relate to renal function. However, there may also be relevant differences between PIs, which are among the most likely agents to be included in nucs-sparing strategies. In new data from a large U.S. Medicaid database queried for relative tolerability of PIs, substantial differences were observed across organ systems (Juday T et al. As presented at EACS 2011. Abstract PE9.1/3). In this study, data from 10 geographically-dispersed Medicaid state programs were analyzed. The study subjects were PI-naive HIV patients between the ages of 18 and 64 who were initiating LPV, DRV, boosted or unboosted atazanavir (ATV), or fosamprenavir (FPV). Although all patients received at least two NRTIs, the types of NRTIs were similar across the PI groups. For each patient, medical claims were evaluated grouped across common adverse events.
As the success of regimens with a single boosted-PI or a PI with another non-NRTI agent is highly dependent on good compliance and long-term tolerability, selecting an agent with a relatively low likelihood of exacerbating an age-related morbidity is likely to be important.
While there were minor differences in many adverse events, such as lipodystrophy, which was <0.5% for all four PIs, relative differences in others were marked. In particular, claims regarding renal-related adverse events were 8.6% for DRV versus less than 3.5% for all three other PIs. Claims for diabetes were 9.5% for DRV, 6% for ATV, 5.7% for FPV, but only 2.4% for LPV. Claims for dyslipidemia were 9.5% for DRV, 5.2% for ATV, 3.6% for FPV, and 1.5% for LPV, or a more than six-fold difference between DRV and LPV (Fig. 2). In the context of treatment overall, these differences may be highly relevant to choices for aging HIV patients particularly in the context of nucs-sparing strategies. As the success of regimens with a single boosted-PI or a PI with another non-NRTI agent is highly dependent on good compliance and long-term tolerability, selecting an agent with a relatively low likelihood of exacerbating an age-related morbidity is likely to be important.
New EACS Guidelines: Role for PIs
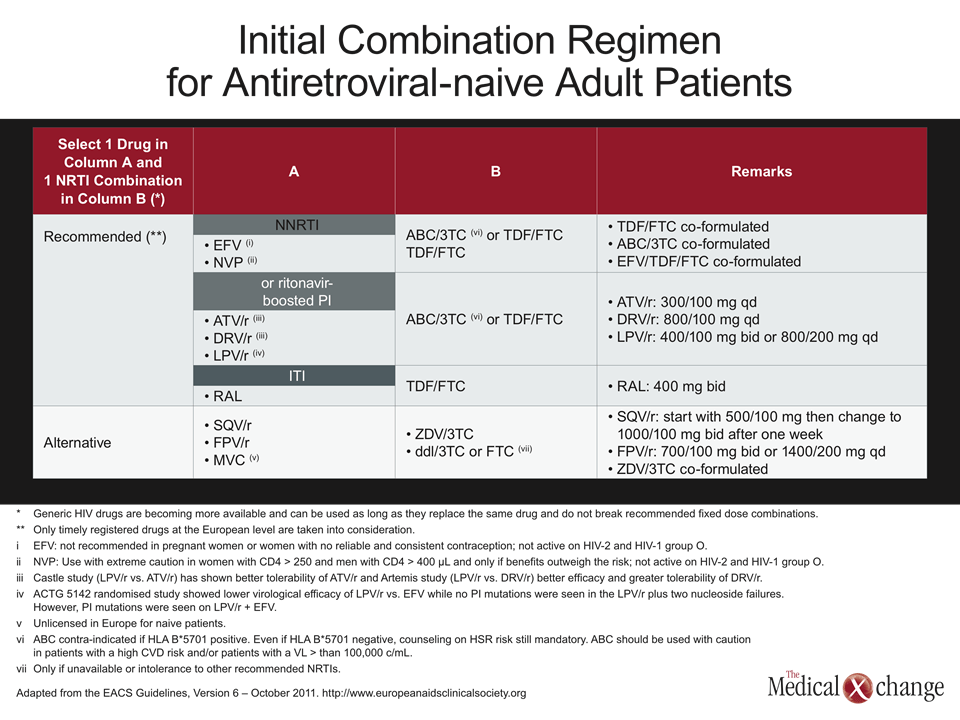
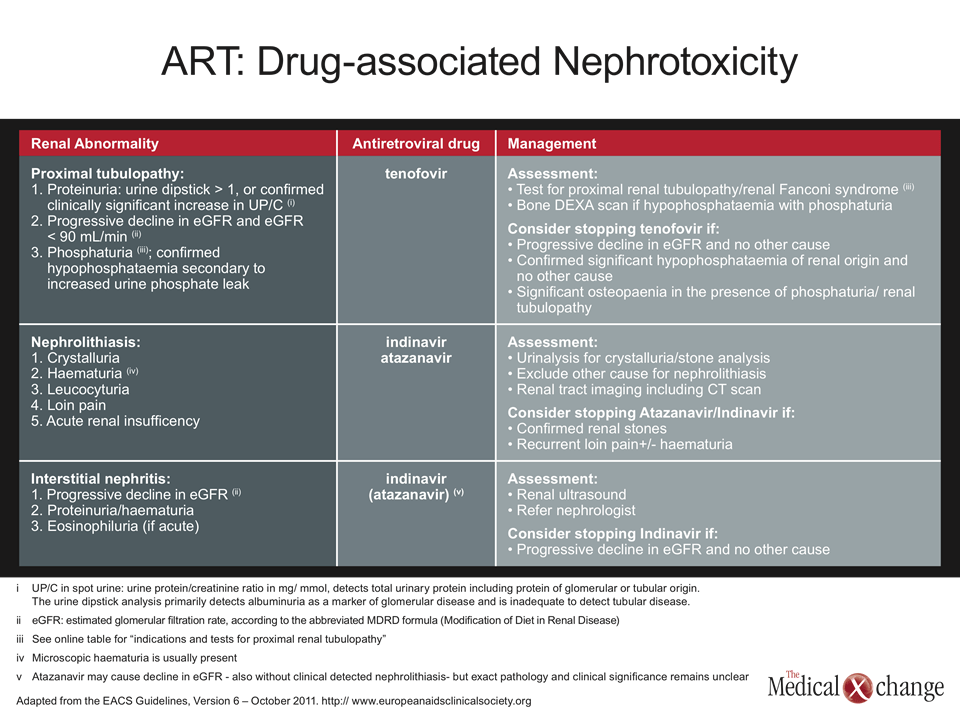
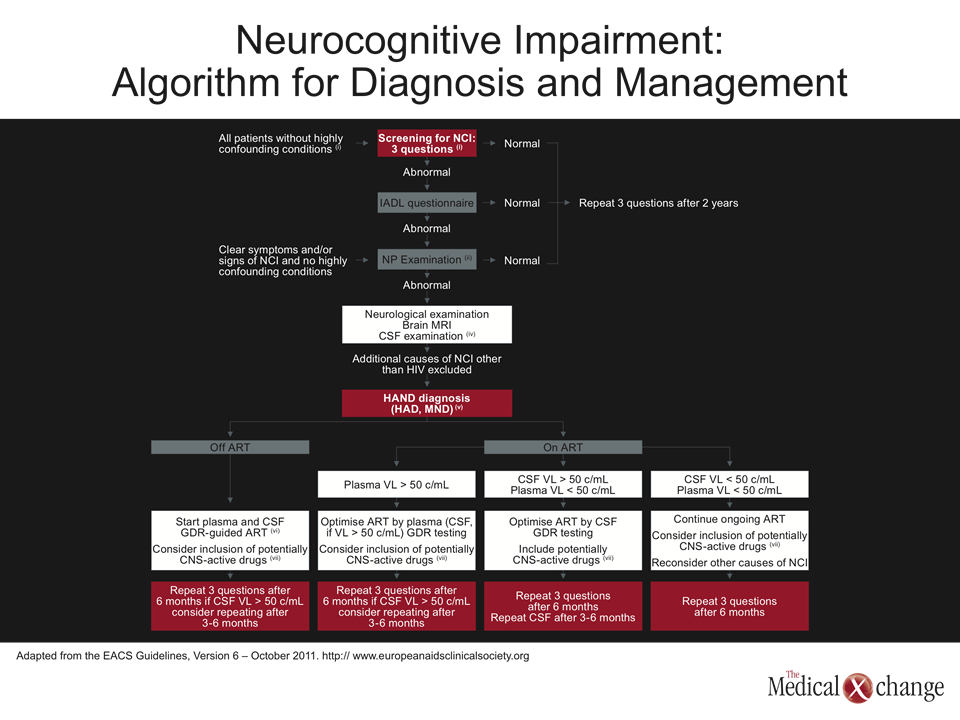
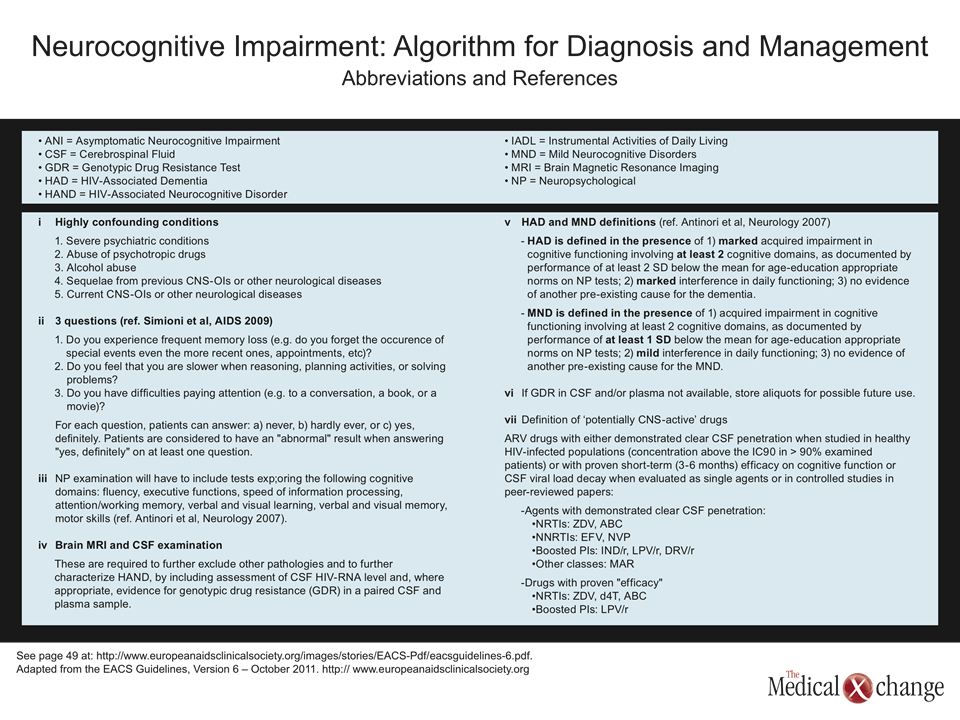
The release and distribution of the latest EACS Guidelines at the 2011 meeting (Version 6 – October 2011, available at www.europeanaidsclinicalsociety.org) was long awaited. The comprehensive guide, which is divided into four parts, including sections on assessment, treatment, prevention of non-infectious co-morbidities, and management of hepatitis co-infection. These sections cover most of the critical issues in contemporary care of the HIV patient. It is notable in the context of PIs, that LPV/r, DRV/r, and ATV/r remain, along with the non-nucleoside reverse transcriptase inhibitors (NNRTIs) and integrase inhibitors as recommended anchors of initial combination therapy with two NRTIs (Table 2). In assessing other strategies, the guidelines identify monotherapy with LPV/r or DPV/r as an option in patients with intolerance to NRTI or for treatment simplification when viral loads have been <50 copies/mL for at least the previous six months. In evaluating specific issues of organ function, whether or not related to aging, the new Guidelines also provide specific guidance on treatment selection for a variety of non-infectious complications. In relation to PIs, for example, ATV and indinavir (IDV) are singled out as risk factors for nephrolithiasis and interstitial nephritis, indicating that these agents should be avoided in patients with or at risk for renal impairment (Table 3). For neurocognitive impairment, the guidelines point out that the only PIs with proven penetration of the cerebrospinal fluid (CSF) are LPV, DRV, and IDV. However, the LPV/r was the only PI identified as having proven efficacy for neurocognitive impairment. These types of detailed recommendations in regard to organ dysfunction are becoming critically important to management as HIV patients age.
Conclusion
In the treatment of HIV, no single issue is more important than sustained viral suppression, but the current selection of potent antiretroviral therapies is permitting more simplified strategies to be considered. The role of nucs-sparing regimens is still being defined, but there is a growing body of evidence that nucs sparing is viable and can avoid the toxicities of NRTIs, including lipodystrophies, and provide substantial relief to the drug budget. For individualized therapy, nucs-sparing PI regimens may also be important in aging individuals trying to minimize treatment-related risks for CVD, renal impairment, and impaired bone metabolism. Multicentre nucs-sparing studies, such as the PROGRESS study with LPV/r and RAL, are helping to establish a role for these strategies in routine patient management.
Additional Slides
Figure 3 (Fig. 3), 4 (Fig. 4), 5 (Fig. 5) and 6 (Fig. 6).
Protease Inhibitors in Nucs-Sparing Strategies: Report from the EACS
Belgrade – Antiretroviral combinations that do not include nucleoside reverse transcriptase inhibitors (NRTIs; ‘nucs’), so-called nucs-sparing regimens, were once largely tested as a strategy to avoid mitochondrial toxicities. However, this approach now offers promise in reducing some of the specific age-related morbidities exacerbated by NRTIs, such as progressive renal impairment. It could also save costs. At the 13th European AIDS Clinical Society (EACS) meeting, a variety of new information was presented on the role of protease inhibitors (PIs) in nucs-sparing regimens. Whether combined with another PI or a drug from another class, such regimens were reported as already being in routine use at some centres even while clinical studies attempt to define which patients are the best candidates. Overall, the data presented suggested that nucs-sparing is a reasonable and appropriate option in at least some select patient groups for whom NRTIs are relatively contraindicated. As more data become available, this approach may beextended to the larger HIV population, including those who are treatment naive.
Show review