Expert Review
39th European Society of Medical Oncology (ESMO) Congress: Expert Review
New Data in Metastatic Castration-resistant Prostate Cancer
Fred Saad, MD, FRCS
Professor and Chief of Urology, Director of G-U Oncology University of Montreal
Endowed Chair in Prostate Cancer Research, Centre Hospitalier de l'Université de Montréal (CHUM)
University of Montreal, Montreal, Quebec
Madrid – The introduction of new therapeutic options for metastatic castration-resistant prostate cancer (mCRPC) is altering strategies for prolonged disease control. New data presented on several of these options at the 2014 European Society for Medical Oncology (ESMO) Congress are relevant to the effort to define how mCRPC treatment is best sequenced. The most significant data were generated from two phase III trials. In one, the latest long-term survival outcomes were made available from the COU-AA-302 trial with abiraterone acetate. In the other, quality of life outcomes were evaluated in the PREVAIL study of enzalutamide. Phase II efficacy and safety data were presented on sipuleucel-T and sorafenib. In addition, a series of studies evaluating prognostic factors and biomarkers provided context for the ongoing effort to determine which treatments should be used in the first-, second- and third-line settings.
Inhibiting Androgen Biosynthesis for Sustained Control
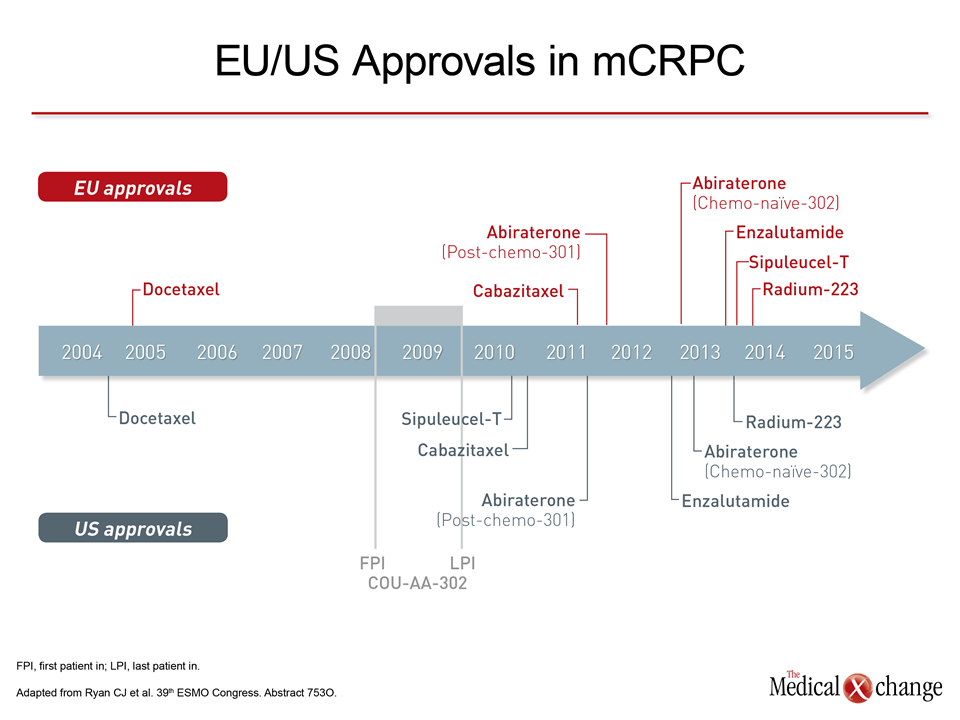
An expanding number of therapeutic agents over the past four years have provided new opportunities to sustain control of metastatic castration-resistant prostate cancer (mCRPC) (Fig. 1). Of these, agents targeted at inhibiting androgen biosynthesis are widely regarded as the most promising. Chemotherapy with docetaxel,1 immunotherapy with sipuleucel-T,2 and radiotherapy with radium-2333 have each been associated with survival benefits in controlled trials, but mCRPC, which is defined by tumour growth despite testosterone levels <7 ng/L, appears to be androgen-dependent. This mechanism therefore provides a greater theoretical opportunity for initial control even if multiple lines of therapy are subsequently required. The benefit of androgen pathway inhibition was initially established with abiraterone acetate, which inhibits cytochrome P-450c17, an enzyme critical to androgen synthesis in the testes. Similar studies followed with enzalutamide, which inhibits the androgen receptor. The landmark COU-AA-301 trial enrolled patients previously treated with docetaxel and associated abiraterone acetate with a significant overall survival (OS) benefit relative to placebo, reducing the hazard ratio (HR) of death by 35% (P<0.001).4 In a comparable trial with enzalutamide administered in patients previously treated with docetaxel, the improvement in OS was similar (HR 0.63; P <0.001).5
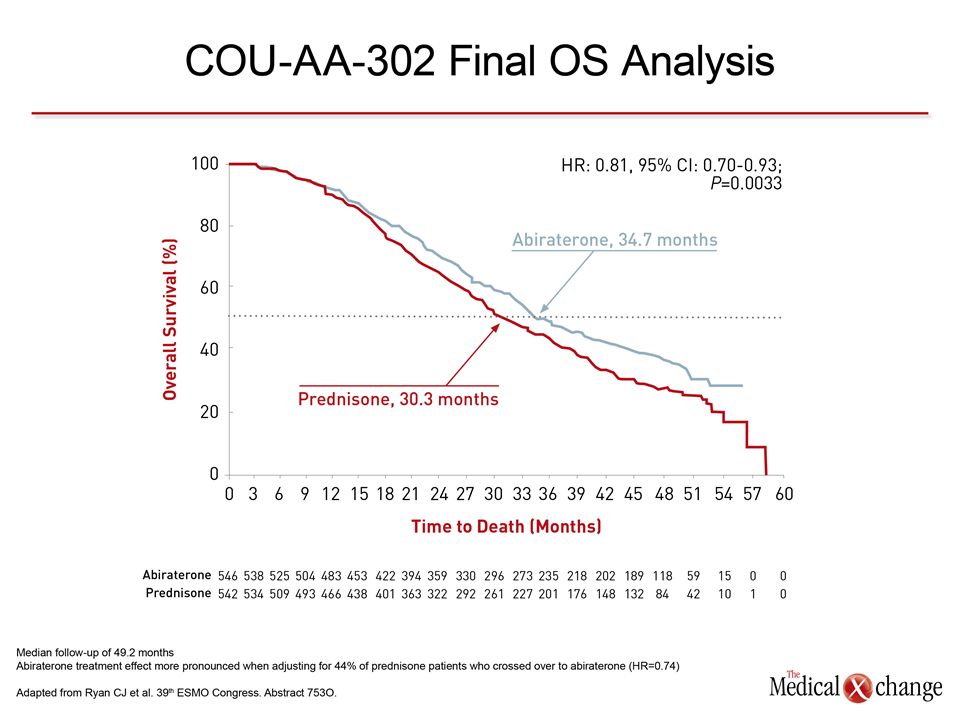
With a median follow-up that has now reached 49.2 months, the OS benefit of abiraterone relative to prednisone (HR 0.81; P=0.0033) remains sustained.
Based on preliminary evidence,6,7 two subsequent studies demonstrated efficacy from androgen pathway inhibitors initiated prior to chemotherapy. In the COU-AA-302 trial with abiraterone acetate, which was stopped for efficacy after an interim analysis, the HR for OS was 0.75 (P=0.01) in favour of abiraterone acetate, relative to an active control arm of prednisone.8 In PREVAIL, also stopped for efficacy at an interim analysis, the HR for OS was 0.71 (P<0.001) in favour of enzalutamide relative to placebo.9 Both studies demonstrated highly-significant benefits on other clinically-important end points such as progression-free survival (PFS).
ESMO: Updated and Final Survival Data
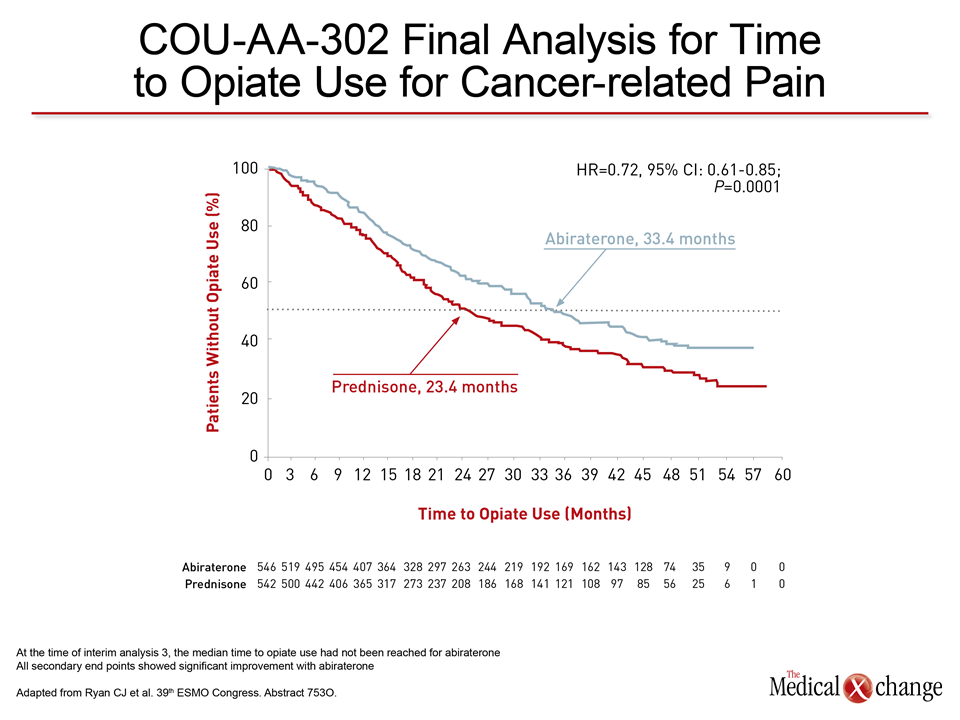
Updated and final survival analyses from the COU-AA-302 trial were presented at the European Society for Medical Oncology (ESMO) 2014 Congress.10 With a median follow-up that has now reached 49.2 months, the OS benefit of abiraterone acetate relative to prednisone (HR 0.81; P=0.0033) remains sustained, producing a more than four-month median survival advantage (34.7 vs. 30.3 months) (Fig. 2) and (Fig. 3). This survival benefit was achieved despite the fact that 44% of patients initially randomized to prednisone crossed over to the abiraterone acetate arm. In addition, the most recent data associate abiraterone acetate with an almost doubling of radiographic PFS (rPFS) relative to prednisone (16.5 vs. 8.2 months; P<0.0001). Moreover, it significantly increased the time to opiate use for cancer-related pain, reducing the risk for this outcome by 28% (P<0.0001) and increasing the mean time to opiates by nearly one year (33.4 vs. 23.4 months) (Fig. 4).
Safety, Tolerability and Quality of Life
The safety and tolerability profile of abiraterone acetate in this extended follow-up was reassuring. Relative to prednisone there were only moderate increases in oedema (31% vs. 24%), hypokalemia (19% vs. 13%), and cardiac disorders (23% vs. 18%). Hypertension was more common on abiraterone acetate (24% vs. 14%), but grade ≥3 levels of this or any other adverse event were uncommon and not significantly different between treatment.
This study provides the most mature analysis of benefit from an agent that inhibits androgen biosynthesis, supporting its value in first-line therapy.
Previously-published data have correlated the clinical outcomes in COU-AA-302 with improved quality of life (QoL).11 In an analysis of Functional Assessment of Cancer Therapy-Prostate (FACT-P), abiraterone acetate has highly-significant improvement (P=0.005) in pain interference and a significantly slower (P=0.005) decline in ECOG performance status score. This study provides the most mature analysis of benefit from an agent that inhibits androgen biosynthesis, supporting its value in first-line therapy. Similar follow-up is not yet available from the PREVAIL trial with enzalutamide, but two PREVAIL sub-studies were presented here. In one, the goal was to evaluate the impact of enzalutamide on QoL, including skeletal-related events (SRE).12 In the other, the analysis was of efficacy in the subset of 204 patients (11.9% of the total) in PREVAIL with visceral disease.13 In a post-hoc analysis of PREVAIL patients who entered the study with visceral disease, the difference in OS for the active therapy and placebo arms did not reach significance (HR 0.82; 95% CI: 0.55-1.23), but there was a significant benefit for rPFS, which was 3.6 months on placebo but not yet reached on enzalutamide (HR 0.28; 95% CI: 0.16-0.49). These data, although only hypothesis-generating, provide initial support for a direct effect of androgen pathway inhibition on visceral disease.
Exploring Alternatives for First-line Strategy
Inhibiting androgen activity in patients with mCRPC is being increasingly accepted as a reasonable first-line strategy, but alternatives continue to be explored. In a randomized phase II study, the tyrosine kinase inhibitor (TKI) sorafenib was tested in 51 men with mCRPC who had developed resistance to prior docetaxel therapy.14 Relative to best supportive care (BSC), sorafenib achieved an objective response or stable disease in 33.3% of patients vs. 7.4% for placebo (P=0.024). Although a small OS advantage did not reach significance, the median PFS was 100 days with sorafenib vs. 89 days with BSC (P=0.019). Another phase II trial, called STRIDE, evaluated the combination of enzalutamide and sipuleucel-T.15 Patients with minimally-symptomatic or asymptomatic mCRPC were randomized to receive enzalutamide two weeks prior or 10 weeks after initiating sipuleucel-T. The study failed to show any effect from the timing of enzalutamide on the peripheral T-cell immune response, which was the primary endpoint, but the study is representative of the growing number of novel strategies being pursued to determine whether sequencing of treatment can extend response.
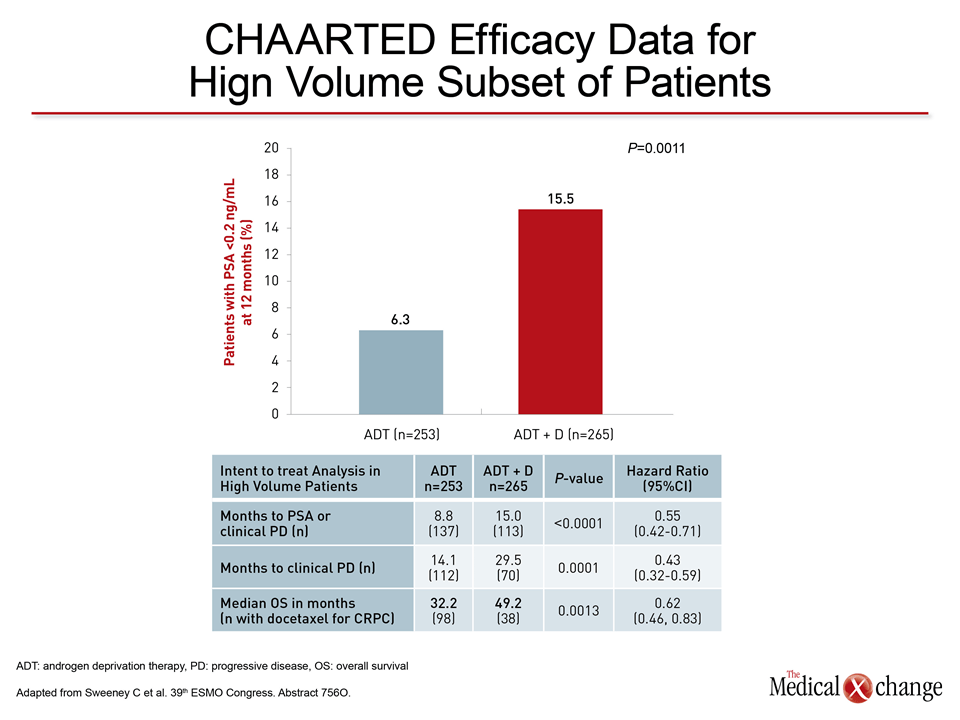
An update of the CHAARTED trial, which was first presented at the 2014 annual meeting of the American Society of Clinical Oncology, suggested that the optimal timing of docetaxel may even be before prostate cancer becomes castration resistant.
Two studies attempting to identify the optimal timing of docetaxel treatment may be more clinically relevant. One, a retrospective study, found no significant difference in OS (38.6 vs. 31.4 months) when patients were treated first with abiraterone acetate and second with docetaxel when compared to the reverse.16 In this study, which had a mean 2.7 years of follow-up, 161 patients received abiraterone acetate first and 37 patients received docetaxel first. The second study, an update of the CHAARTED trial, which was first presented at the 2014 annual meeting of the American Society of Clinical Oncology,17 suggested that the optimal timing of docetaxel may even be before prostate cancer becomes castration resistant.18 In CHAARTED, conducted in 790 men with mCRPC, the addition of docetaxel to androgen deprivation therapy (ADT) increased median OS to 57.6 months from 44 months in those who received ADT alone (P=0.0003). In the ESMO data, the analysis was restricted to the 518 men with high-volume disease. In these, the median OS climbed from 32.2 months on ADT alone to 49.2 months (P=0.0013) on the combination (Fig. 5).
Sequencing mCRPC Therapy
The CHAARTED data underscore the potential for timing of treatments to substantially increase response rates and survival, but prognostic features or patient characteristics may also be important for determining which therapies to use first and when to switch therapies in order to sustain disease control. Several preliminary studies addressed this question at ESMO. In one, PSA response was assessed in several of the major clinical trials with androgen pathway inhibitors, including COU-AA-302 and PREVAIL.19 The study suggested PSA measurement is an independent prognostic variable potentially useful for early monitoring of treatment response. Other studies attempt to identify biomarkers of treatment resistance.
A positive assay for AR- V7 was found to be a sensitive predictor of an inferior PSA response and shorter OS.
Of these biomarkers, one of the most promising, particularly in regard to monitoring androgen pathway inhibitors, may be the androgen receptor splice variant-7 (AR V-7). In a study presented here, a positive assay for AR-V7 was found to be a sensitive predictor of an inferior PSA response and shorter OS, regardless of whether patients were taking abiraterone acetate or enzalutamide.20 The authors cautioned that data are preliminary, but they are reflective of a broader effort to determine when to switch treatments over the course of progressive disease.
Summary
The final OS analysis from the COU-AA-302 as well as data from the PREVAIL trial establish abiraterone acetate and enzalutamide as reasonable first-line therapeutic options for the treatment of mCRPC. However, data presented at ESMO emphasize the ongoing efforts to understand how the growing array of therapeutic options is best sequenced to maximize long-term survival. A rational and systematic approach may emerge if biomarkers prove helpful in characterizing disease activity and the relative value of existing therapies.
Additional Slides
Figures 6 (Fig. 6) and 7 (Fig. 7).
References
1. Tannock IF et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med 2004;351:1502-12. 2. Kantoff PW et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med 2010;363:411-22. 3. Parker C et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med2013;369:213-23. 4. de Bono JS, et al. Abiraterone acetate and increased survival in metastatic prostate cancer. N Engl J Med 2011;364:1995-2005. 5. Scher HI, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 2012;367:1187-97. 6. Attard G et al. Selective inhibition of CYP17 with abiraterone acetate acetate is highly active in the treatment of castration-resistant prostate cancer. J Clin Oncol : official journal of the American Society of Clinical Oncology 2009;27:3742-8. 7. Scher HI, et al. Antitumour activity of MDV3100 in castration-resistant prostate cancer: a phase 1-2 study. Lancet2010;375:1437-46. 8. Ryan CJ, et al. Abiraterone acetate in metastatic prostate cancer without previous chemotherapy. N Engl J Med 2013;368:138-48. 9. Beer TM, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014;371:424-33. 10. Ryan CJ, Smith MR, Fizazi K, Miller K. Final overall survival (OS) analysis of COU-AA-302, a randomized phase 3 study of abiraterone acetate acetate (AA) in metastatic castration-resistant prostate cancer (mCRPC) patients without prior chemotherapy. 39th ESMO 2014. Abstract 7530. 11. Rathkopf DE, et al. Updated Interim Efficacy Analysis and Long-term Safety of Abiraterone acetate Acetate in Metastatic Castration-resistant Prostate Cancer Patients Without Prior Chemotherapy (COU-AA-302). Eur Urol. 2014 Epub ahead of print Mar 6. 12. Loriot Y, Miller K, Sternberg CN, Fizazi K. Impact of enzalutamide on skeletal-realted events, pain, and quality of life in the PREVAIL trial. 39th ESMO 2014. Abstract 762P. 13. Higano CS, Alumkal J, Chowdhury S, Loriot Y. Response rates and outcomes with enzalutamide for patients with metastatic castration resistant prostate cancer and visceral disease in the PREVAIL trial. 39th ESMO 2014. Abstract 767P. 14. Kramer G, Maj-Hes A, Hobisch A, Shariat SF. Multicenter, randomized, double-blind phase II study of srafenib compared to placebo with best supportive care after failure of docetaxel in metastatic castration-resistant prostate cancer. 39th ESMO 2014. Abstract 773P. 15. Petrylak DP, Quinn DI, Dreicer R, Antonarakis ES. STRIDE, a randomized, phase 2, open-label study of sipuleucel-T with concurrent versus sequential enzalutamide in metastatic castration-resistant prostate cancer. 39th ESMO 2014. Abstract 774P. 16. Zafeiriou Z, Ferraldeschi R, Omlin A, Pezaro C. Sequencing docetaxel and abiraterone acetate acetate for metastatic castration-resistant prostate cancer. 39th ESMO 2014. Abstract 791P. 17. Sweeney C, Chen Y, Carducci M, Liu G. Impact on overall survival with chemohormonal therapy versus hormonal therapy for hormone-sensitive newly metastatic prostate cancer; an ECOG-led phase III randomized trial. American Society of Clinical Oncology; 2014; Chicago, USA: Abstract LBA-2. 18. Sweeney C, Chen Y, Carducci M, Liu G. Chemohormonal therapy versus hormonal therapy for hormone naive high volume newly metastatic prostate cancer: ECOG led phase III randomized trial. 39th ESMO 2014. Abstract 7560. 19. Fuerea AC, Baciarello G, Massard C, Abiges Sauvin L. Early PSA response is an independent prognostic factor in patients with mCRPC treated with next-generation androgen pathway inhibitors. 39th ESMO 2014. Abstract 796P. 20. Antonarakis ES, Lu C, Wang H, Luber B. AR-V7 splice variant and resistance to enzalutamide and abiraterone acetate in men with metastatic castration-resistant prostate cancer: overall survival results. 39th ESMO 2014. Abstract 7980.
New Data in Metastatic Castration-resistant Prostate Cancer
Madrid – The introduction of new therapeutic options for metastatic castration-resistant prostate cancer (mCRPC) is altering strategies for prolonged disease control. New data presented on several of these options at the 2014 European Society for Medical Oncology (ESMO) Congress are relevant to the effort to define how mCRPC treatment is best sequenced. The most significant data were generated from two phase III trials. In one, the latest long-term survival outcomes were made available from the COU-AA-302 trial with abiraterone acetate. In the other, quality of life outcomes were evaluated in the PREVAIL study of enzalutamide. Phase II efficacy and safety data were presented on sipuleucel-T and sorafenib. In addition, a series of studies evaluating prognostic factors and biomarkers provided context for the ongoing effort to determine which treatments should be used in the first-, second- and third-line settings.
Show review