Expert Review
Pursuing the Next Step in Reduction of Residual CV Risk
Chapter 3: LDL-C Remains the Single Best Target for CV Risk Reduction
Milan Gupta, MD, FRCPC, FACC
Associate Clinical Professor of Medicine, McMaster University,
Assistant Professor of Medicine, University of Toronto,
Medical Director, Canadian Cardiovascular Research Network,
Toronto, Ontario
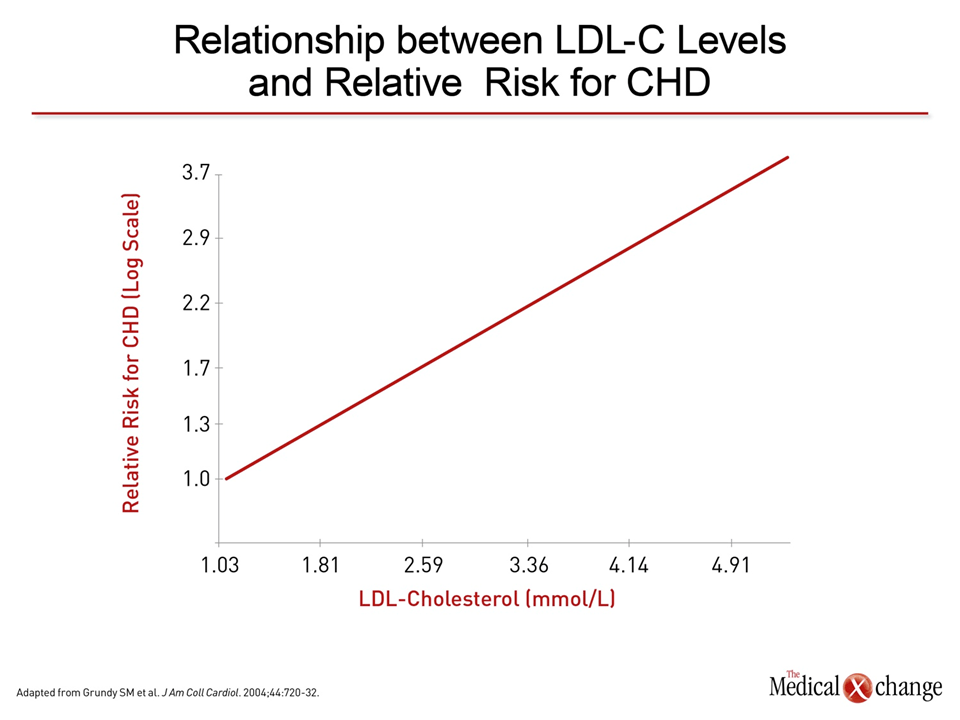
When data from large lipid-lowering trials are aggregated, the relationship between reduction in low-density lipoprotein cholesterol (LDL-C) and risk of cardiovascular (CV) events has been described as log linear.1 With some variability, there is about a 1% reduction in CV risk for each 1% reduction in LDL-C (Figure 1). Reductions of this magnitude have been reported with statins, non-statins, surgery and diet.2 Although there is a need for more potent lipid-lowering therapies to increase the proportion of high-risk patients who reach guideline-defined targets for LDL-C, the point at which reduction in LDL-C provides no additional reduction in CV risk has yet to be defined. It is reasonable to determine whether treating LDL-C beyond current guideline targets provides additional protection against CV events, particularly in high-risk individuals.
Background
According to the lipid hypothesis, elevated blood levels of LDL-C are a treatable and fundamental mediator of atherosclerosis. A large body of evidence has been accumulated to support this hypothesis. Much of this data has been derived from multicenter statin trials, which have repeatedly associated large LDL-C reductions with major reductions in CV events. In the 14-trial meta-analysis performed by the Cholesterol Treatment Trialists’ (CTT) Collaboration, which included data from approximately 90,000 randomized patients, each 1 mmol/L reduction in LDL-C was associated with a 23% reduction in CV risk (Fig. 1).3
Clinical Trial Programs
Due to the fact that the preponderance of evidence supporting the benefits of LDL-C lowering was derived from statin trials, drugs within this class have been identified as the first-line option in Canadian guidelines.4 This is appropriate on the basis of both the efficacy and the favourable tolerability profile of statins, but assertions that benefits are unique to these agents are refuted by several studies. For example, a meta-analysis that included 5 trials of diet, 3 trials of bile acid sequestrants, 1 trial of surgery (partial ileal bypass) and 10 statin trials found that the reduction in CV risk relative to LDL-C reduction was consistently proportional across the methodologies to achieve these reductions.2
A meta-analysis that included 5 trials of diet, 3 trials of bile acid sequestrants, 1 trial of surgery and 10 statin trials found the reduction in CV risk relative to LDL-C reduction was consistently proportional across methodologies to achieve these reductions.
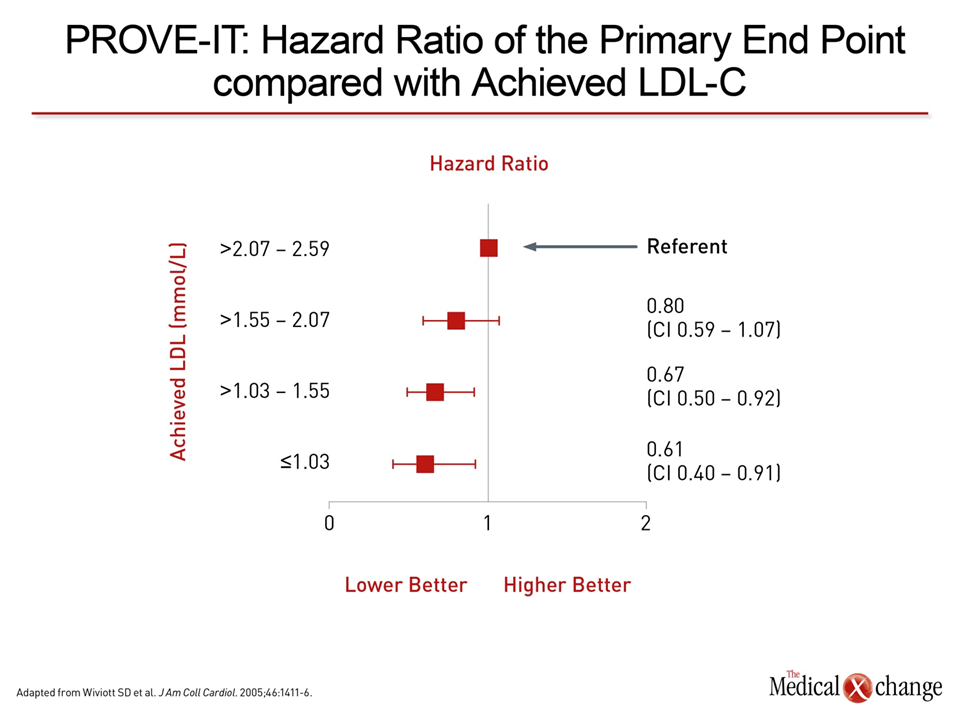
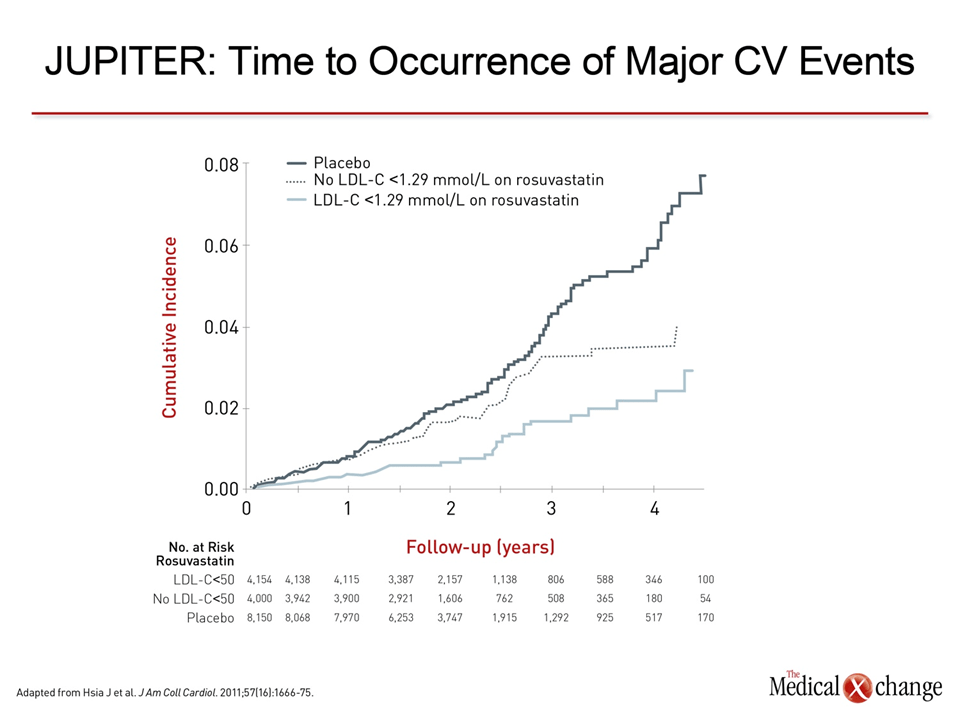
The lower is better adage for LDL-C in relation to CV risk reduction is based on a history of clinical trials that have each shown a lower LDL-C level to be advantageous relative to a higher level. In the initial trials, pre-treatment LDL-C levels were relatively high, particularly by current standards. In the Scandinavian Simvastatin Survival Study (4S), for example, the average LDL-C at entry was nearly 5.0 mmol/L.5 While this study associated a nearly 40% reduction in LDL-C relative to placebo with a 34% reduction in CV events, subsequent studies, such as PROVE-IT and Treating to New Targets (TNT),6,7 enrolled patients with much lower LDL-C levels at entry and still demonstrated large CV risk reductions commensurate with relative reductions in LDL-C on treatment. Although fewer trials have been conducted with non-statins, the lower is better principle has been relatively consistent with only rare exceptions, such as the HPS2-THRIVE study, which did not associate niacin with CV risk reduction.8 The largest non-statin trial ever conducted, IMPROVE-IT, was recently completed.9 In this trial, ezetimibe was compared to placebo in 18,144 very high-risk patients (enrolled within 10 days of hospitalization for an acute coronary syndrome) taking simvastatin. Relative to simvastatin alone, the addition of ezetimibe produced a 22% further reduction in LDL-C, which was associated with a 6.4% reduction (P=0.016) in risk of a composite endpoint of CV death, non-fatal myocardial infarction (MI), unstable angina requiring hospitalization, revascularization, and non-fatal stroke after a median of 6 years of follow-up. The IMPROVE-IT data expanded evidence that LDL-C lowering with non-statin therapies achieves statistically significant CV risk reductions. Although the reduction in risk was somewhat less than that predicted by the reduction in LDL-C relative to previous trials, end-of-study LDL-C levels were the lowest ever achieved in the comparator arm of a large multicenter trial. In the group receiving simvastatin plus ezetimibe, the median time-weighted average LDL-C at end of study was 1.4 mmol/L. In the comparator arm, the average LDL-C was 1.8 mmol/L. Both meet or exceed the Canadian guideline target of ≤2.0 mmol/L for high-risk patients.4 These data draw attention to the potential for LDL-C reduction below current guideline-defined targets to provide even greater CV risk protection, particularly in the very high-risk patients enrolled in IMPROVE-IT. The evidence-based Canadian guidelines define targets that are near the maximum LDL-C reductions currently achieved with available lipid-lowering therapies. However, the potential for even lower LDL-C levels to provide additional CV risk reductions has yet to be evaluated. While IMPROVE-IT demonstrates a relative risk protection for 1.4 mmol/L relative to higher levels of LDL-C, exploratory analyses conducted with data from several studies suggest benefit from even lower levels. For example, 45% of the approximately 2,000 patients randomized to the experimental arm of PROVE-IT, which was the first trial to demonstrate an advantage for a high-intensity relative to more moderate statin therapy,6 achieved LDL-C levels <1.55 mmol/L. When patients in the experimental arm were stratified into quartiles, a stepwise further reduction in CV events was observed for each 0.5 mmol/L increment reduction in LDL-C below 2.0 mmol/L in a published post-hoc analysis (Fig. 2).10 There was no safety signal observed for very low LDL-C across several types of adverse events, such as those involving liver or muscle function. Similarly, the TNT trial, which associated an average LDL-C of 2.0 mmol/L with a major reduction in CV risk relative to an average LDL-C of 2.6 mmol/L in the comparator arm,7 provided data on 6,107 patients who achieved LDL-C levels below 1.5 mmol/L. When these were stratified, a post-hoc analysis again showed a trend for a mortality benefit for those with an LDL-C of 1.0 mmol/L but <2.0 mmol/L.11 In the JUPITER trial, which randomized 17,802 apparently healthy individuals to a high-intensity statin or placebo,12 a post-hoc study compared the risk reduction in the 4,000 patients on a high-intensity statin that achieved LDL-C 1.3 mmol/L.13 Both levels of LDL-C provided a significant risk reduction relative to placebo even though this was a population with moderate CV risk, but the lower LDL-C was associated with an incremental additional risk reduction relative the higher LDL-C (Fig. 3). In an analysis of adverse events, the authors reported no differences in rates of muscle-related side effects, cancer, diabetes, or neuropsychiatric conditions.
All of these data suggest that lower is better with no point identified at which further relative reductions do not appear to provide further relative protection.
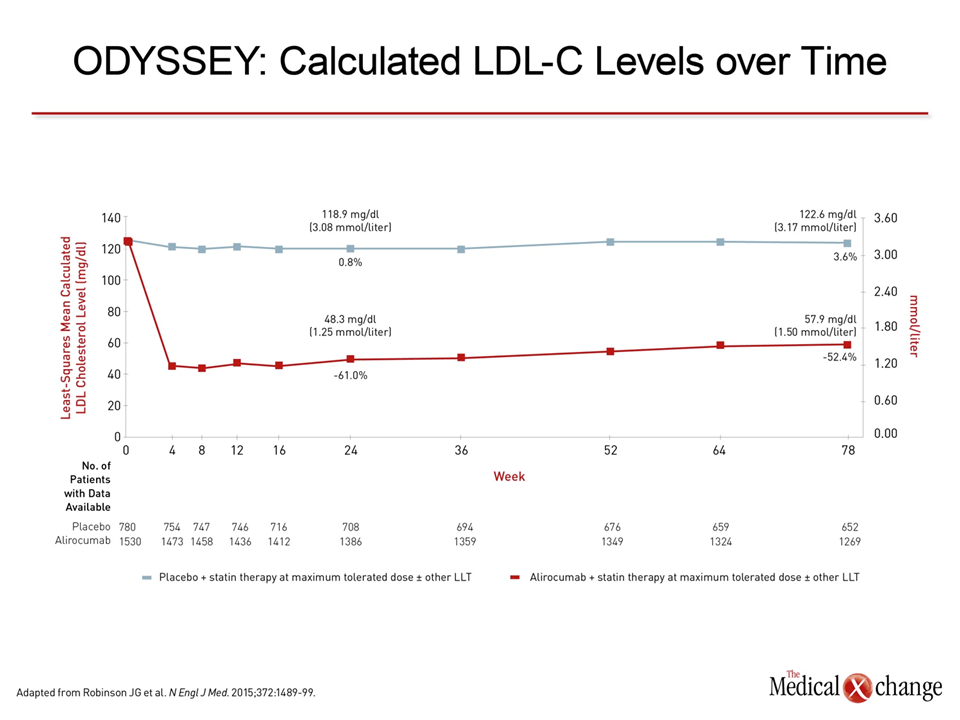
All of these data suggest that lower is better with no point identified at which further relative reductions do not appear to provide further relative protection. Based on experimental evidence and epidemiologic studies conducted in populations consuming low-fat diets, such as hunter-gatherers, it has been speculated that the appropriate physiological level of LDL-C in humans is in the range of 1.3 to 1.8 mmol/L.14 However, physiologic levels may not be the appropriate target in patients with existing atherosclerosis. This is suggested by the continuum of benefit at very low levels suggested by the previously cited post-hoc trial analyses. Although published studies have made an association between very low LDL-C and an increased risk of a broad array of adverse events, including cancer,15 suicide,16 and intracranial hemorrhage,17 these risks are not consistent across sets of data, including the safety analyses from PROVE-IT, TNT, and JUPITER. More recent data with the PCSK9 inhibitors provide additional evidence that very low LDL-C levels are safe and efficacious in regard to CV risk protection. In the ODYSSEY Long-Term trial, which randomized 2,341 high-risk patients to the PCSK9 inhibitor alirocumab or placebo on top of maximally-tolerated statins, alirocumab provided a 62% additional reduction in LDL-C at the end of 24 weeks relative to maximally-tolerated statins alone (Fig. 4).18 Longer follow-up is needed to evaluate relative protection against CV events, but a favourable trend at 78 weeks consistent with this reduction in LDL-C was reported. The large reductions in LDL-C that can be achieved on PCSK9 inhibitors provide an opportunity to further explore the limits of the lower-is-better hypothesis. In ODYSSEY Long-Term, the average LDL-C was 1.1 mmol/L after 24 weeks on treatment. Of the 1,550 patients receiving this therapy, 38% achieved LDL-C <0.65 mmol/L of which nearly half achieved LDL-C levels <0.4 mmol/L. In a detailed safety analysis presented at the 2015 annual meeting of the American College of Cardiology (ACC), this was characterized as one of the largest evaluations of patients with pharmacologically-induced LDL-C levels this low.19 In this analysis, no meaningful imbalances were observed in musculoskeletal, neurologic, or gastrointestinal disorders, and the author concluded that no specific signals of safety risks were detected. However, the longer-term safety of achieving such low LDL-C levels remains to be confirmed. In the open-label OSLER 1 and 2 trials with the PCSK9 inhibitor evolocumab, LDL-C was reduced 61% from baseline to a median on-treatment LDL-C of 1.25 mmol/L.20 Again, a favourable trend toward reduced risk of major CV events commensurate with the reductions in LDL-C was observed on the PCSK9 inhibitor relative to placebo, while safety data remained reassuring. In this study, 37.1% of patients achieved a LDL-C <0.65 mmol/L. The rate of adverse events and types of adverse events were comparable in this subgroup relative to those with higher LDL-C levels. These studies are sufficiently large to permit further exploratory analyses regarding the premise that lower is better when long-term follow-up is completed and CV events are adjudicated. Like data from the post-hoc analyses conducted with data from PROVE-IT, TNT, and JUPITER, lower event rates corresponding with lower LDL-C stratifications, if observed, will not prove lower is better. Rather, it will be another step in the journey toward defining optimal LDL-C targets in high-risk patients. Trials will be needed both to confirm an incremental advantage for the extremely low LDL-C levels possible on PCSK9 inhibitors as well as evaluate relative safety. Such large outcome trials are underway with several PCSK9 inhibitors in high-risk patients.
Summary
Incremental reductions in LDL-C in clinical trials have been nearly uniformly associated with incremental reductions in risk of CV events in high-risk patients. Current guidelines based on these trials have identified targets but do not define the optimal level of LDL-C to achieve maximum reduction in CV risk. Despite high-intensity statin therapy, very low levels of LDL-C have not been a realistic goal in most high-risk individuals, but a new generation of therapies with greater LDL-C lowering efficacy may provide the opportunity to finally identify the level at which protection from CV risk is safely optimized.
References
1. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J Am Coll Cardiol 2004;44:720-32. 2. Robinson JG, Smith B, Maheshwari N, Schrott H. Pleiotropic effects of statins: benefit beyond cholesterol reduction? A meta-regression analysis. J Am Coll Cardiol 2005;46:1855-62. 3. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267-78. 4. Anderson TJ, Gregoire J, Hegele RA, et al. 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol 2013;29:151-67. 5. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-9. 6. Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004;350:1495-504. 7. LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005;352:1425-35. 8. Group HTC, Landray MJ, Haynes R, et al. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med 2014;371:203-12. 9. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med 2015;372:2387-97. 10. Wiviott SD, Cannon CP, Morrow DA, et al. Can low-density lipoprotein be too low? The safety and efficacy of achieving very low low-density lipoprotein with intensive statin therapy: a PROVE IT-TIMI 22 substudy. J Am Coll Cardiol 2005;46:1411-6. 11. Leeper NJ, Ardehali R, deGoma EM, Heidenreich PA. Statin use in patients with extremely low low-density lipoprotein levels is associated with improved survival. Circulation 2007;116:613-8. 12. Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359:2195-207. 13. Hsia J, MacFadyen JG, Monyak J, Ridker PM. Cardiovascular event reduction and adverse events among subjects attaining low-density lipoprotein cholesterol <50 mg/dl with rosuvastatin. The JUPITER trial (Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin). J Am Coll Cardiol 2011;57:1666-75. 14. O’Keefe JH, Jr., Cordain L, Harris WH, Moe RM, Vogel R. Optimal low-density lipoprotein is 50 to 70 mg/dl: lower is better and physiologically normal. J Am Coll Cardiol 2004;43:2142-6. 15. Benn M, Tybjaerg-Hansen A, Stender S, Frikke-Schmidt R, Nordestgaard BG. Low-density lipoprotein cholesterol and the risk of cancer: a mendelian randomization study. J Natl Cancer Inst 2011;103:508-19. 16. Ellison LF, Morrison HI. Low serum cholesterol concentration and risk of suicide. Epidemiology 2001;12:168-72. 17. Noda H, Iso H, Irie F, et al. Low-density lipoprotein cholesterol concentrations and death due to intraparenchymal hemorrhage: the Ibaraki Prefectural Health Study. Circulation 2009;119:2136-45. 18. Robinson JG, Farnier M, Krempf M, et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med 2015;372:1489-99. 19. Robinson JG, Farnier M, Chaudhari U. Adverse evets in patients with low-density lipoprotein cholesterol levels <25 or <15 mg/dL on at least two consecutive visits in 14 randomized, controlled, clinical trials of alirocumab. American College of Cardiology. San Diego 2015. 20. Sabatine MS, Giugliano RP, Wiviott SD, et al. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N Engl J Med 2015;372:1500-9.
Chapter 3: LDL-C Remains the Single Best Target for CV Risk Reduction
When data from large lipid-lowering trials are aggregated, the relationship between reduction in low-density lipoprotein cholesterol (LDL-C) and risk of cardiovascular (CV) events has been described as log linear.1 With some variability, there is about a 1% reduction in CV risk for each 1% reduction in LDL-C (Figure 1). Reductions of this magnitude have been reported with statins, non-statins, surgery and diet.2 Although there is a need for more potent lipid-lowering therapies to increase the proportion of high-risk patients who reach guideline-defined targets for LDL-C, the point at which reduction in LDL-C provides no additional reduction in CV risk has yet to be defined. It is reasonable to determine whether treating LDL-C beyond current guideline targets provides additional protection against CV events, particularly in high-risk individuals.
Show review