Expert Review
Pursuing the Next Step in Reduction of Residual CV Risk
Chapter 1: Lipid Lowering: The Road to Current Treatment Guidelines
Jean C. Grégoire, MD, FRCPC, FACC
Cardiologist Montreal Heart Institute Associate Professor of Medicine
Université de Montréal, Montreal, Quebec
On the basis of randomized trials over the past 2 decades, the treatment goals for low-density lipoprotein cholesterol (LDL-C) have been lowered repeatedly. In Canada, the current LDL-C goal for patients with high risk of cardiovascular (CV) events is ≤2.0 mmol/L or a ≥50% reduction from a pre-treatment level.1 This represents a practical target for LDL-C reductions, even though the level of LDL-C with no additional CV risk reductions has yet to be defined. Whether or not newer, more effective therapies for control of LDL-C provide the evidence for another, yet still-lower LDL-C target, many Canadians with established CV disease or a risk equivalent are not at current goals. The reasons are varied, but such individuals represent a missed opportunity to avoid CV events and CV-associated mortality.
Background
The evidence that LDL-C is a treatable risk factor for CV events predates the introduction of HMG-CoA reductase inhibitors (statins). In 1984, the Lipid Research Clinics – Coronary Primary Prevention Trial (LRC-CPPT) associated a 12.6% reduction in LDL-C with a 19% reduction in coronary heart disease (CHD) death or non-fatal myocardial infarction (MI) over a median follow-up of 7.4 years.2 In that placebo-controlled study, which enrolled more than 3800 men, the study agent was the bile acid sequestrant cholestyramine. The data from that study was employed to conclude that LDL-C might play a causal role in the pathogenesis for heart disease. The lipid hypothesis has largely evolved into the lipid principle of CV risk management over many years of large trials with statins, a relatively well-tolerated and convenient therapy that facilitated treatment. The first of these large trials, the Scandinavian Simvastatin Survival Study (4S), associated a 35% reduction in LDL-C with a 42% reduction in coronary deaths and a 30% reduction in all-cause mortality after a median follow-up of 5.4 years.3 In this secondary prevention study, simvastatin was compared to placebo in 4444 men and women with a previous MI or angina pectoris. The landmark secondary and primary prevention trials that followed generated equally impressive reductions in CV risk. The earliest of these studies, such as the West of Scotland Coronary Prevention Study (WOSCOPS)4 and the Heart Protection Study (HPS),5 compared a statin to placebo. Subsequent studies, such as the Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction 22 (PROVE IT–TIMI 22) trial and the Treating to New Targets (TNT) trial,6,7 compared more aggressive to less aggressive lipid lowering. Each study supported the principle that lower is better in regard to LDL-C. Many of these trials were influential in defining new and lower LDL-C targets for a series of revised treatment guidelines developed in Canada and elsewhere.
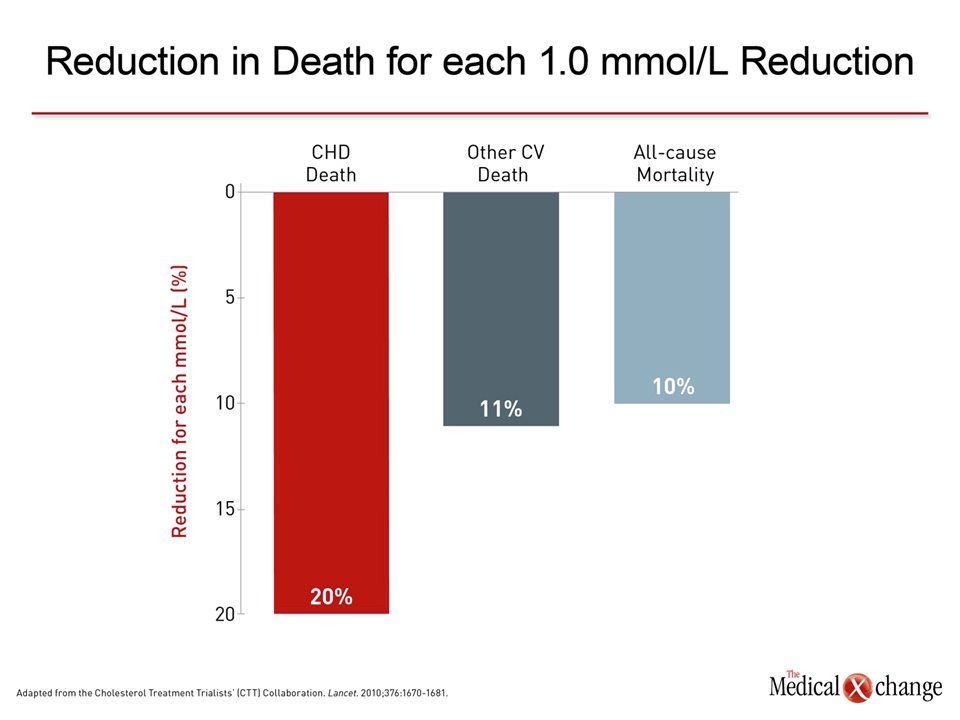
Each 1.0 mmol/L reduction in LDL-C is associated with a 20% reduction in deaths due to coronary heart disease.
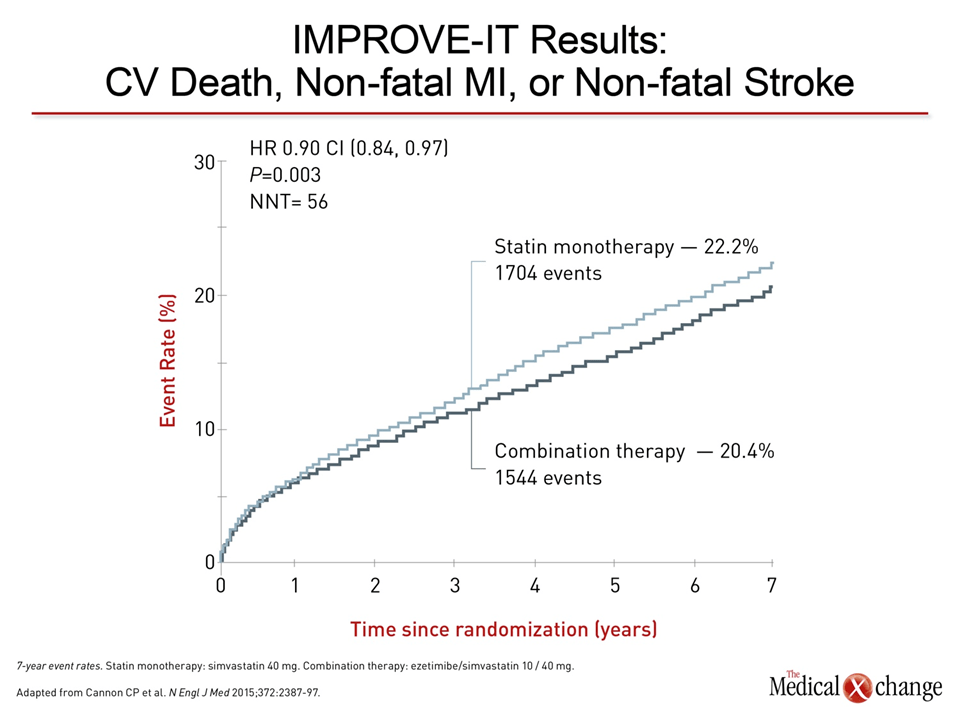
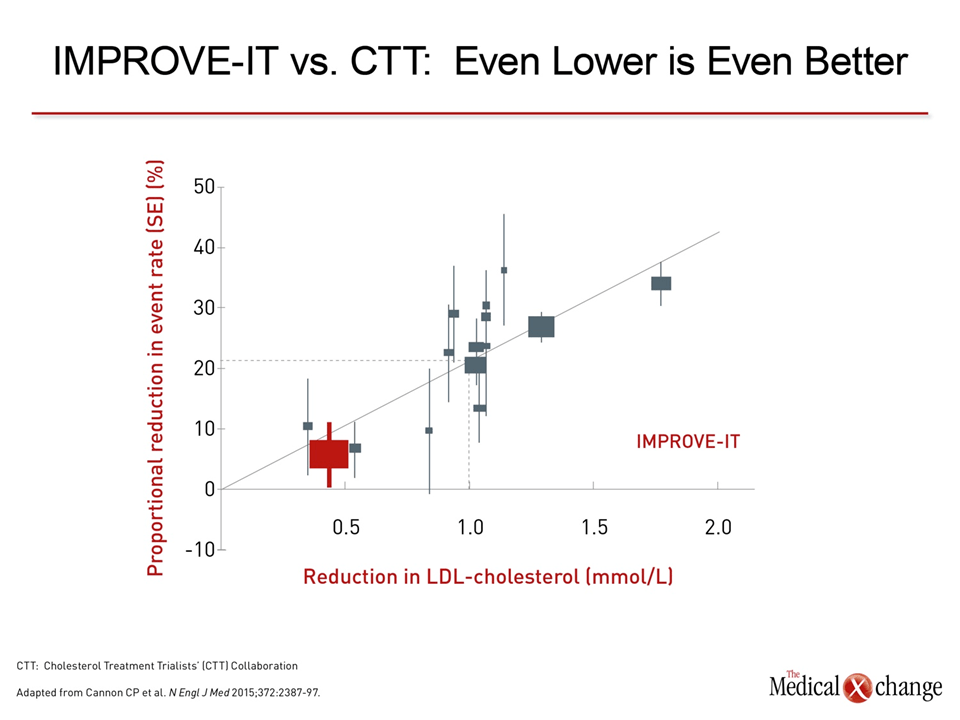
On the basis of data consolidated from 26 controlled statin trials that randomized at least 1000 patients and had at least 2 years of follow-up, it was estimated that each 1.0 mmol/L reduction in LDL-C is associated with a 20% reduction in deaths due to coronary heart disease, an 11% reduction in deaths due to other cardiac causes, and a 10% reduction in all cause-mortality (Fig. 1).8 In this meta-analysis, performed by the Cholesterol Treatment Trialists’ Collaboration (CTT), no significant association was made between relative reductions in LDL-C and increase risk of death from non-vascular causes, including cancer. Due to the preponderance of data in which CV risk reductions were achieved with LDL-C lowering on statins, Canadian and other treatment guidelines have emphasized the use of agents within this class. However, LDL-C reductions with non-statins, such as those seen with cholestyramine in the LRC-CPPT trial and diet in smaller studies, suggest that similar reductions are achieved with non-statins.2,9 A recently published multinational trial also suggested that combining a non-statin with a statin provides additional reductions in both LDL-C and CV events relative to a statin alone.10 In that study, called Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), an additional 0.4 mmol/L reduction in LDL-C achieved with ezetimibe relative to simvastatin alone was associated with a 6.64% reduction in a composite CV endpoint that included MI, hospitalization for angina, or revascularization. For the endpoint of CV death, non-fatal MI, or non-fatal stroke, the risk reduction was 10% with the addition of ezetimibe (Fig. 2). The risk reduction, although modest, is consistent with the expected CV risk reduction that was established in the CTT meta-analysis (Fig. 3).
Guidelines and Treatment Success
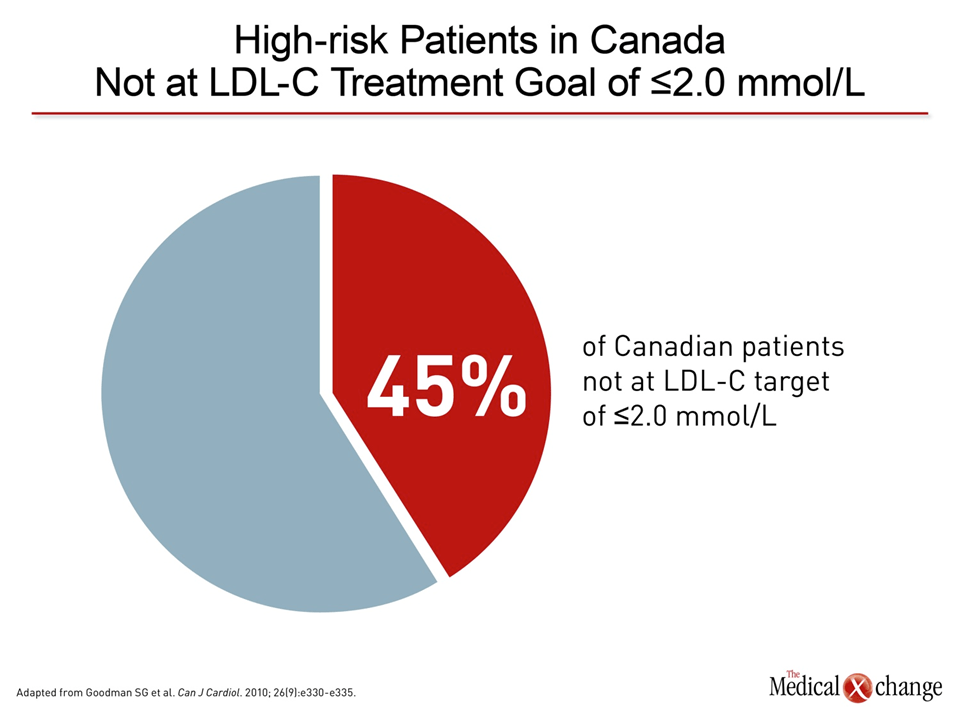
A substantial proportion of individuals in Canada at high risk of CV events, including those who have already had a CV event, are not at the current LDL-C treatment goal. In a cross-sectional study of 2436 outpatients 45 years of age or older who were taking a statin, 45% of those who met high-risk criteria were not at the treatment goal established by the Canadian Cardiovascular Society (CCS) in the 2006 guidelines (Fig. 4).11 In a multinational study of patients with diabetes mellitus that included more than 1000 Canadian participants, only 40% were at LDL-C goal despite statin treatment.12 In both of these studies, statin doses were frequently low, but the list of reasons for failing to reach guideline targets in these studies was varied and included poor tolerance to statins, lack of adequate lipid lowering on maximally tolerated high intensity statins, failure of physicians to titrate statins to reach the guideline target, and lack of adherence. The proportion of patients who should be at an evidence-based guideline goal but are not has been referred to as a care gap. Although such patients face an avoidable risk of life-threatening complications, care gaps are complex. Each of the reasons patients fail to reach goals is likely to be multifactorial and not necessarily easily derived from objective data. For example, there has been a large disparity between trial-defined and clinically reported intolerance to statins. In a meta-analysis of 44 atorvastatin trials, the overall incidence of myalgias was 1.9% (versus 0.8% for placebo),13 but cohort studies from large databases suggest muscle-related adverse events in up to 20% of patients,14 complicating efforts to understand the causes of discontinuation outside of clinical trials.
Approximately 50% of patients prescribed a statin discontinue therapy in the first year.
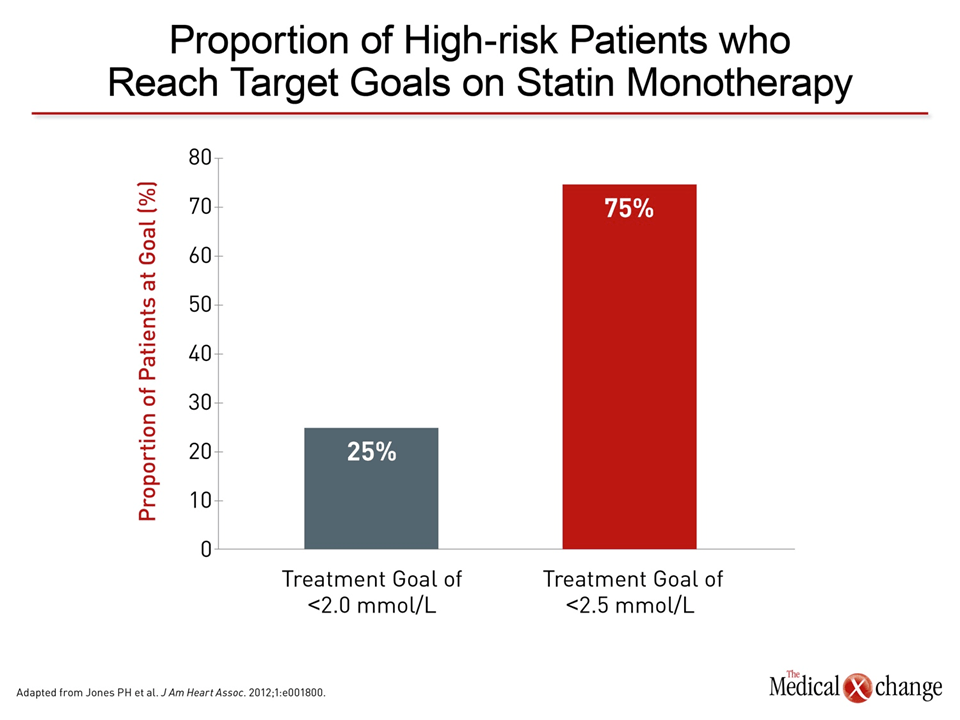
High intensity statins, such as atorvastatin and rosuvastatin, are capable of achieving LDL-C reductions from pre-treatment levels of approximately 50% when used at the upper level of the recommended dose range, but maximally tolerated dose is a subjective term in an empirical sense. Some degree of muscle symptoms on statins have been reported in up to 29% of patients, and many of these individuals discontinue therapy, switch therapy, reduce their dose of therapy, or use therapy inconsistently.15 In addition, many high-risk patients are unable to reach the current relatively aggressive treatment goals on statin monotherapy. In one study that employed data from healthcare databases, only 25% had reached the treatment goal of <2.0 mmol/L even though nearly 75% of patients reached the target of <2.5 mmol/L (Fig. 5).16
There is evidence that physicians who place high-risk patients on statins do not initiate therapy at sufficient doses or confirm that targets have been met.
There is evidence that physicians who place high-risk patients on statins do not initiate therapy at sufficient doses or confirm that targets have been met. In a study that evaluated statin prescriptions in patients hospitalized for an acute coronary syndrome, almost all were treated with statin, but only 52% received a high intensity statin.17 In the previously cited Canadian study of high-risk males in which only 45% were at goals, nearly 90% had been prescribed atorvastatin or rosuvastatin, but doses were intermediate or low.11 In a retrospective review of more than 9000 patients with coronary artery disease, only 37% on statin monotherapy were at the treatment goal, but 41% of those on statins were taking regimens with only moderate potency.18 In high-risk patients who have not yet had a CV event or for those who do not fully appreciate the relationship between elevated LDL-C and risk of a recurrent event, adherence may be another obstacle to treatment goals. Approximately 50% of patients prescribed a statin discontinue therapy in the first year.19 Although these data include both low- and high-risk patients, a claims database study found adherence was slightly lower on high- relative to low-intensity statins.20 In a study of Medicare beneficiaries, 80% of patients who were on a high intensity statin prior to hospitalization for CHD filled a prescription for a high intensity statin after discharge, but only 23.1% filled a high intensity prescription if they had not been on a statin previously. Inadequate adherence to evidence-based therapy is a well-recognized barrier to optimal risk reduction for many types of cardiovascular therapies, such as blood pressure lowering medications,21 but the large CV risk reductions anticipated from statins predict the toll in morbidity and mortality from non-adherence to these agents to be particularly high.22
How to Improve
The care gap, which defines the distance between the current rate of CV events and the substantially lower rate of events if all high-risk patients were at LDL-C goals, is not likely to be fully closed, but it could be reduced. Several strategies are required. Most important, current treatment options should be applied for optimal effect. This not only includes encouraging physicians to employ high intensity statins at maximally tolerated doses, but to educate patients about the goals of therapy and to encourage adherence even in the event of bothersome but benign adverse events. It also includes greater willingness among both patients and physicians to employ non-statin therapies adjunctively when goals are not reached on statins alone. Ezetimibe, which is well tolerated, has been rendered an evidence-based option on the basis of the IMPROVE-IT trial. Reductions in all-cause mortality observed in some clinical trials as well as the CTT meta-analysis provides the ultimate test and proof of the critical role played by LDL-C lowering in CV risk management. The development of new therapies that provide greater reduction of LDL-C either as an alternative to statins or when combined with statins will certainly extend the large risk reductions to those who are not now achieving treatment goals on available therapies. The phase 3 trials with the proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors suggest drugs within this class may fulfill this role. These and other agents may also allow new, even lower targets of LDL-C to be evaluated for their ability to prevent CV events.
Summary
In high-risk individuals, evidence-based guidelines define treatment goals for LDL-C associated with major reductions in both CV events and overall mortality. The evidence that a substantial proportion of such individuals are not at goals suggests a need to revisit and revise strategies that will reduce untreated risk. New treatment options that can be used adjunctively or in place of statins would be expected to reduce this care gap, but there is also likely to be a substantial opportunity for an improvement in outcomes from better use of existing treatments.
References
1. Anderson TJ, Gregoire J, Hegele RA, et al. 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol 2013;29:151-67. 2. The Lipid Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of coronary heart disease. JAMA 1984;251:351-64. 3. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-9. 4. Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 1995;333:1301-7. 5. Heart Protection Study Collaborative G. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 2002;360:7-22. 6. Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004;350:1495-504. 7. LaRosa JC, Grundy SM, Waters DD, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005;352:1425-35. 8. Cholesterol Treatment Trialists C, Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010;376:1670-81. 9. Robinson JG, Smith B, Maheshwari N, Schrott H. Pleiotropic effects of statins: benefit beyond cholesterol reduction? A meta-regression analysis. J Am Coll Cardiol 2005;46:1855-62. 10. Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med 2015;372:2387-97. 11. Goodman SG, Langer A, Bastien NR, et al. Prevalence of dyslipidemia in statin-treated patients in Canada: results of the DYSlipidemia International Study (DYSIS). Can J Cardiol 2010;26:e330-5. 12. Leiter LA, Berard L, Bowering CK, et al. Type 2 diabetes mellitus management in Canada: is it improving? Can J Diabetes 2013;37:82-9. 13. Newman CB, Palmer G, Silbershatz H, Szarek M. Safety of atorvastatin derived from analysis of 44 completed trials in 9,416 patients. Am J Cardiol 2003;92:670-6. 14. Newman CB, Tobert JA. Statin intolerance: reconciling clinical trials and clinical experience. JAMA 2015;313:1011-2. 15. Wei MY, Ito MK, Cohen JD, Brinton EA, Jacobson TA. Predictors of statin adherence, switching, and discontinuation in the USAGE survey: understanding the use of statins in America and gaps in patient education. J Clin Lipidol 2013;7:472-83. 16. Jones PH, Nair R, Thakker KM. Prevalence of dyslipidemia and lipid goal attainment in statin-treated subjects from 3 data sources: a retrospective analysis. J Am Heart Assoc 2012;1:e001800. 17. Shiu JR, Pearson GJ, Charrois TL, Gyenes G, Koshman SL. Frequency of intensive statin therapy in patients with acute coronary syndrome admitted to a tertiary care center. Am J Cardiol 2012;109:1-5. 18. Karalis DG, Victor B, Ahedor L, Liu L. Use of Lipid-Lowering Medications and the Likelihood of Achieving Optimal LDL-Cholesterol Goals in Coronary Artery Disease Patients. Cholesterol 2012;2012:861924. 19. Mann DM, Woodward M, Muntner P, Falzon L, Kronish I. Predictors of nonadherence to statins: a systematic review and meta-analysis. Ann Pharmacother 2010;44:1410-21. 20. Virani SS, Woodard LD, Akeroyd JM, Ramsey DJ, Ballantyne CM, Petersen LA. Is high-intensity statin therapy associated with lower statin adherence compared with low- to moderate-intensity statin therapy? Implications of the 2013 American College of Cardiology/American Heart Association Cholesterol Management Guidelines. Clin Cardiol 2014;37:653-9. 21. Calvert SB, Kramer JM, Anstrom KJ, Kaltenbach LA, Stafford JA, Allen LaPointe NM. Patient-focused intervention to improve long-term adherence to evidence-based medications: a randomized trial. Am Heart J 2012;163:657-65 e1. 22. Lardizabal JA, Deedwania PC. Benefits of statin therapy and compliance in high risk cardiovascular patients. Vasc Health Risk Manag 2010;6:843-53.
Chapter 1: Lipid Lowering: The Road to Current Treatment Guidelines
On the basis of randomized trials over the past 2 decades, the treatment goals for low-density lipoprotein cholesterol (LDL-C) have been lowered repeatedly. In Canada, the current LDL-C goal for patients with high risk of cardiovascular (CV) events is ≤2.0 mmol/L or a ≥50% reduction from a pre-treatment level.1 This represents a practical target for LDL-C reductions, even though the level of LDL-C with no additional CV risk reductions has yet to be defined. Whether or not newer, more effective therapies for control of LDL-C provide the evidence for another, yet still-lower LDL-C target, many Canadians with established CV disease or a risk equivalent are not at current goals. The reasons are varied, but such individuals represent a missed opportunity to avoid CV events and CV-associated mortality.
Show review