Expert Review
Solving Osteoarthritis Pain Control: Current Status of Hyaluronic Acid Knee Injections
Chapter 2: Hyaluronic Acid in the Knee: History, Characteristics and Efficacy
R. Timothy Deakon, MD, FRCSC
Oakville Sports Injury Clinic, Oakville, Ontario
In the knee, hyaluronic acid (HA), a naturally-occurring compound with viscoelastic properties, is credited with several physiologic functions associated with joint homeostasis. This includes a role in compression force distribution, tissue lubrication, and regulation of cellular activities.(1) In patients with osteoarthritis (OA) of the knee, a chronic degenerative process that adversely affects both cartilage and bone,(2) viscosupplementation with exogenously-produced formulations of HA has been available for more than 15 years. Direct comparisons between current products remain limited, but the distinctions between treatments are potentially important for clinical activity. These distinctions, which may influence onset and duration of pain relief as well as safety, include composition, molecular weight, and molecular activity. Consideration of the physiochemical properties of HA may also be relevant to the more challenging goal of slowing or preventing further joint deterioration.
Background
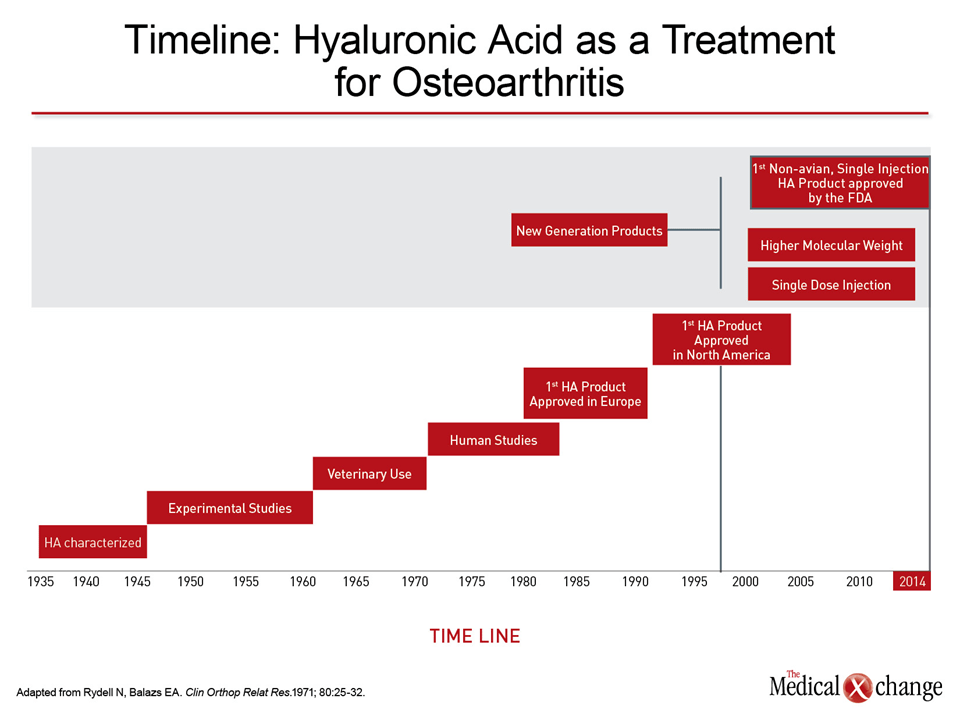
Hyaluronic acid (HA), also referred to as hyaluronan or hyaluronate, is a naturally-occurring viscoelastic glycosaminoglycan polysaccharide with polymeric and polyelectrolyte properties.(3) It is found in a variety of human and animal connective tissues besides joint synovial fluid, such as vitreous body, nasal cartilage, and the skin, where it has been injected for cosmetic purposes.(4) Interest in HA as a treatment for osteoarthritis (OA) dates to the early 1970s when human studies were initiated after evidence of benefit in animals (Fig. 1).(5) Commercial injectable HA products, which are licensed as a medical device, first received regulatory approval in the late 1990s. The initial and subsequent products, which may not be interchangeable as a result of divergent characteristics, have been evaluated in numerous meta-analyses and data reviews.(6,7)
In patients with OA, as well as many other inflammatory joint diseases, the concentration of endogenous HA is reduced, a change consistent with a concomitant reduction in the viscoelastic properties of the synovial fluid.(8) This change may not be just mechanical. A series of human and experimental studies support a role of HA in numerous biological processes, including matrix remodeling and inhibition of damage from activated cytokines.(9) Its role in signal transduction through interaction with the CD44 receptor on the chondrocyte is implicated in cell proliferation, angiogenesis, and cell migration.(10,11) HA may also be involved in mediating pain perception. (12) Various formulations of HA and biological scaffolds dependent on HA have been developed in a variety of tissue engineering studies, including those for bone, ligament, cartilage, and osteochondral defects.(13-15) In knee OA, as in the other applications, the composition of exogenous HA may be relevant to its clinical activity. The ideal characteristics of HA in the OA knee are unknown and may vary for objectives such as modification of pain, the inflammatory response, or viscoelastic mechanical properties. Theoretical advantages have driven the development of products that vary for source of HA extraction, molecular weight, cross-linking and other characteristics with potential relevance to half-life in the joint, dosing, duration of pain relief, safety, and preservation of joint integrity.
HA Development: Differing Properties
The first and many early HA products were extracted from rooster combs, which distinguishes them from the non-avian products later derived from bacterial fermentation. The extraction source is a potential safety issue, leading to labeling for avian products that has established a relative contraindication for patients with known allergies to avian products, including poultry, eggs, or feathers.(16) The relatively low molecular weights of earlier HA formulations also predict lower viscosity,(17) a likely disadvantage for stress distribution. The low relative dose concentrations of early products explain the need for more frequent injections to achieve stable pain control.
Recent HA products, which are less often extracted from avian sources, are being engineered to provide durable activity. Several products now demonstrate pain relief sustained for up to 6 months on a single injection. While this prolonged activity may be related to residence time, there is evidence to suggest that modern formulations may also initiate molecular changes, including favorable effects on chondrocyte and synoviocyte behavior, to sustain clinical benefit. To date, there is no compelling evidence to differentiate HA therapies for disease-modifying effects, but the differences between HA formulations provide a basis for pursuing how properties may alter the underlying disease pathology.
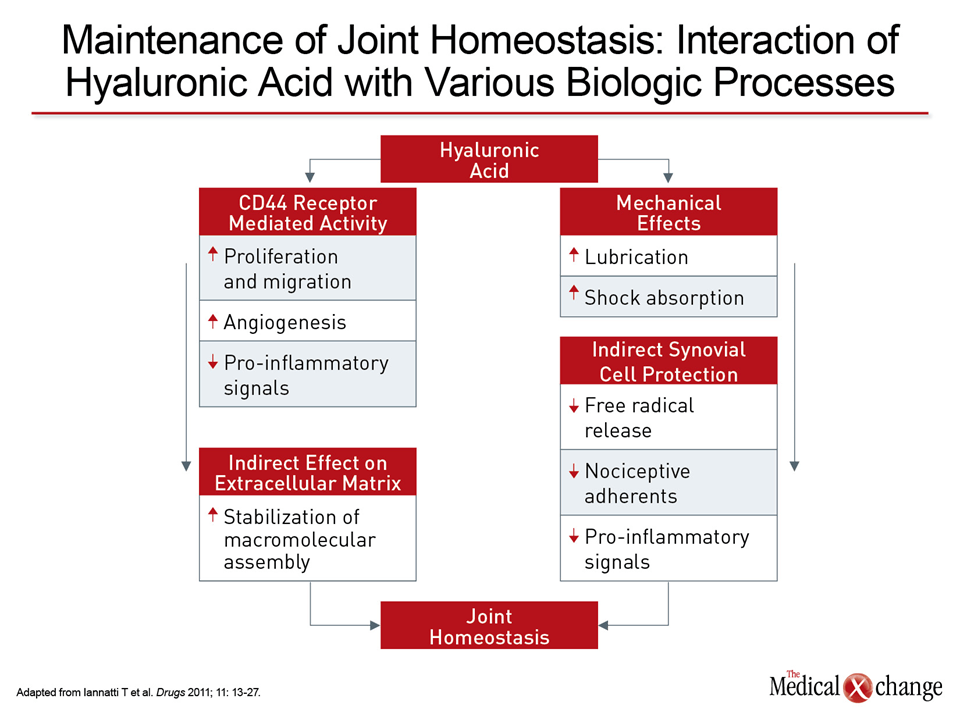
One area of interest is the interaction of HA with the CD44 receptor on chondrocytes as a potentially fundamental step to joint integrity. The CD44 receptor interacts with COX-2,(18) prostaglandins,(18) and osteoblast-mediated osteoclastogenesis,(19) which are all implicated in the homeostasis of joint function. Based on the likelihood that such characteristics as molecular weight affect the ability of HA to interact with CD44, it is reasonable to expect differences in the relative ability of HA formulations to mediate inflammation, extracellular matrix formation, and synovial fluid function (Fig. 2).
Evolution of HA Formulations
The putative goal of HA injections is to restore the viscoelastic properties of synovial fluid which is depleted both in the concentration and the molecular weight of endogenous HA.(10) This is based on the premise that improving the mechanical properties of synovial fluid is the mechanism by which HA relieves symptoms. This may be true, but it has not been proven. Alternatively, there is also interest in developing an exogenous HA capable of recreating the full range of biological activities attributed to naturally occurring HA. This includes a homeostatic role that may involve mediation of events that underlie progressive OA.
In the presence of OA, the normal balance between synthesis of new matrix and degradation of aging cartilage is disrupted.(20) The exact cascade of events leading to this disruption is the focus of intensive investigation, but the loss of HA may exacerbate or even drive the process. HA can be linked to the activity of many, if not all, of the factors suspected of participating in OA, including at least indirect exacerbation of loss of aggrecan, a prostaglandin that participates in the integrity of cartilage and which is degraded early in the course of OA.(21) The potential for HA to exert a protective effect on the cartilage, independent of its ability to restore the viscoelasticity of the synovial fluid, is derived from its ability to bind to the CD44 chondrocyte receptor. While adhesion to the CD44 receptor is associated with chondrocyte proliferation and retention,(22) it is also involved in retaining and anchoring the prostaglandin aggregates important to matrix formation.(23) In experimental studies, HA administration has stimulated production of extracellular matrix proteins such as chondroitin and been associated with increased prostaglandin production.(24,25) Whether a downstream or independent effect, experimental studies have also associated HA with suppression of pro-inflammatory cytokine expression, another factor implicated in progressive OA.(26)
The list of other effects potentially relevant to the homeostatic activity of HA in the knee and the ability of exogenous administration to restore this activity is long and includes protection of chondrocytes against oxidative stress and inhibition of vascular endothelial growth factor (VEGF) and other proteins thought to participate in OA.(27,28) In one set of experiments, cross-talk was demonstrated between HA and inhibitors of COX-2, resulting in a reduction in chondrocyte apoptosis and extending evidence that HA is involved in fundamental molecular pathways mediating joint physiology.(18)
In recreating the effects of endogenous HA for joint homeostasis, there is evidence that molecular weight is a significant variable. In a study of cultured synovial fibroblasts, HA with higher molecular weights produced greater stimulation than HA with lower molecular weights.(29) The authors of this study suggested that exogenous HA of optimal molecular weight may not only exert a greater protective effect but encourage endogenous HA production. In another set of experiments with HA of graded molecular weights, degradation of cartilage and return to a more favorable histology were both improved with higher relative to lower molecular weights.(30,31)
In addition to molecular weight, dose concentration may be one of the most important differentiating characteristics between HA formulations. While a greater volume of active drug per injection has the potential to accelerate the time to drug activity and increase the dwell time, a higher drug concentration may define the ability of one formulation relative to another to both recreate the activities of endogenous HA, but also to stimulate endogenous HA production. In addition to speed and duration of symptom control, these variables may hold the key for developing OA therapies that restore homeostasis and inhibit disease progression.
Clinical Data: Differentiating HA Formulations
There are no large trials to provide objective evidence for a clinically-significant difference between the seven HA products now available in Canada. Recent preference of products that achieve pain control after a single injection is likely to be driven largely by convenience, but newer products based on evolving evidence of favorable HA characteristics, such as relatively high molecular weight, also have theoretical clinical advantages. Trials leading to regulatory approval of these agents have not typically had active comparators, but most of the current devices have labeling that describe an indication for pain relief in patients with OA who have failed to respond to non-pharmacologic therapies or simple analgesics like acetaminophen.
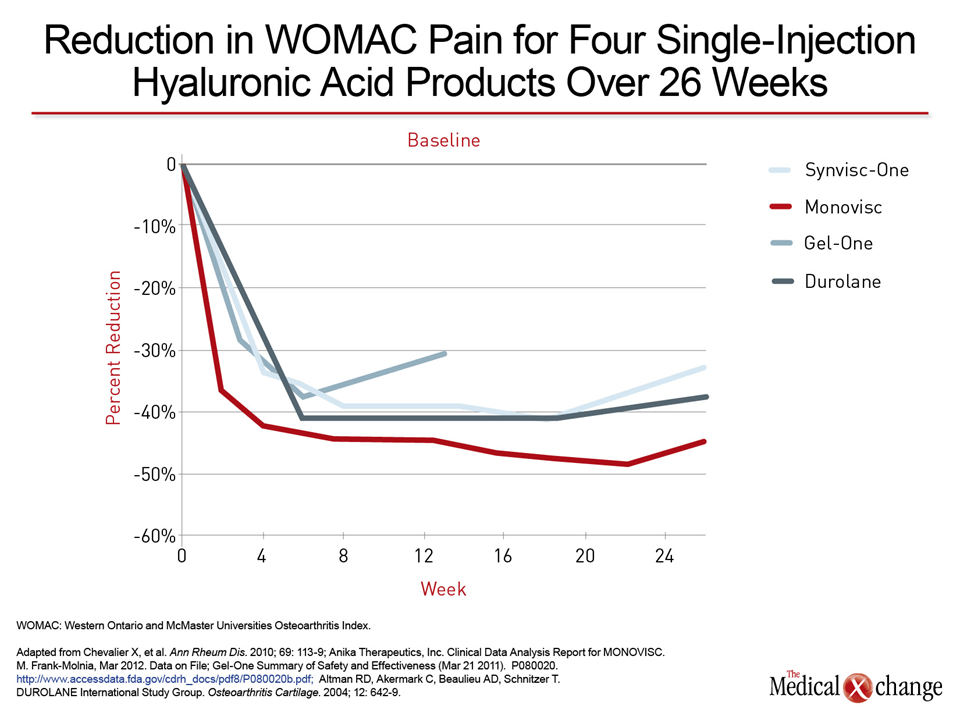
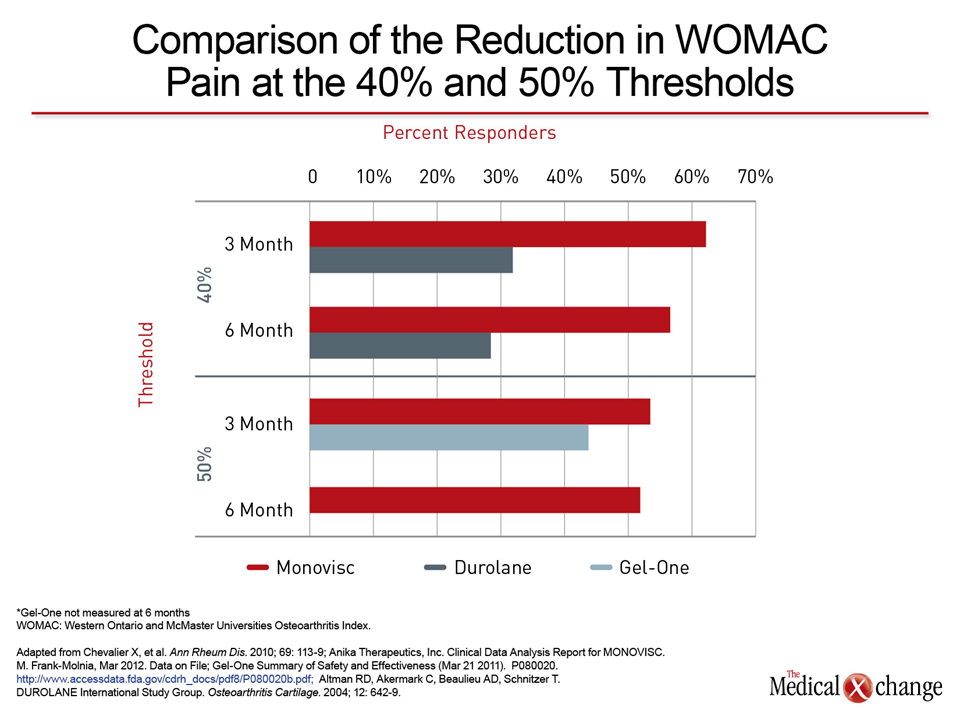
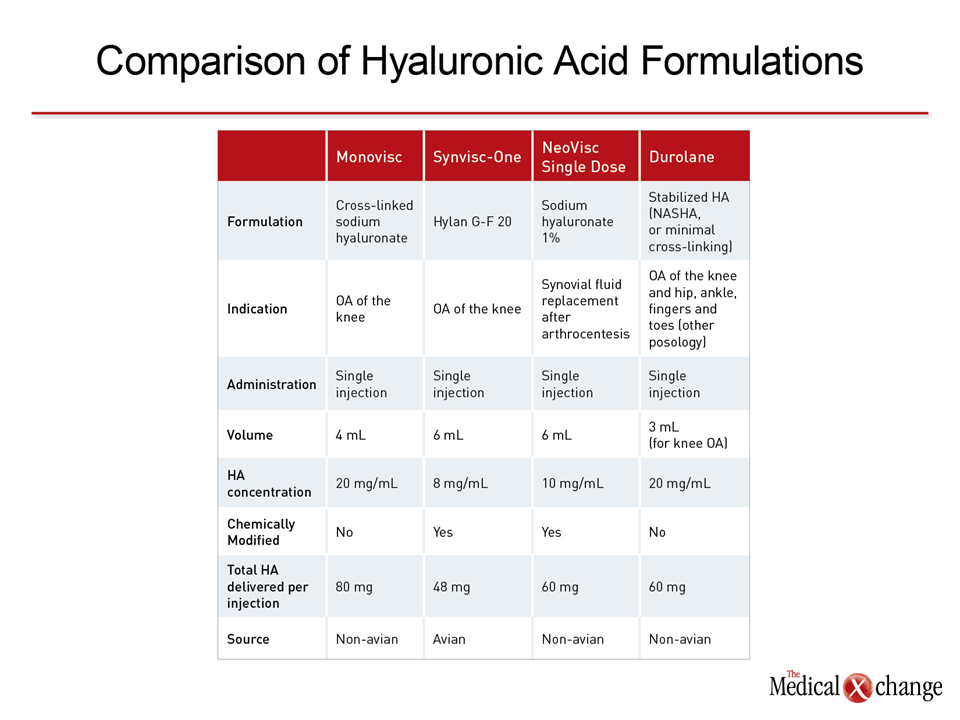
The five single-injection products are Monovisc, Synvisc-One, Gel-One, Neovisc, and Durolane. Multi-injection HA products, like Orthovisc and Synvisc, remain available, but treatments that can be administered with fewer injections are likely to be preferred by patients. Of the single-injection products, Synvisc-One is chemically related to the earlier generation, multidose Synvisc, which is an avian-based product. Gel-One is also avian-based. Monovisc, Durolane, and Neovisc are all non-avian based. Each of these is a member of the most recent generation of HA injection products and has a high molecular weight relative to initial HA formulations. Each has been evaluated in a pivotal, saline-controlled trial with symptomatic relief evaluated out to 26 weeks. From the U.S. Food and Drug Administration (FDA), the current labeling for Monovisc is for the treatment of pain in patients with moderate OA of the knee. Similar labeling has been granted to Synvisc-One, Durolane, and Neovisc. Graphically, non-comparative data indicate that Monovisc may act more rapidly than many of the other current single injection HA formulations (Fig. 3) and (Fig. 4). These data are hypothesis generating in the absence of a randomized trial, but differences in formulation provide an expectation of an unequal onset of action or duration of effect. Relative to other single injection HAs, the dose concentrations are 80 mg for Monovisc, 48 mg for Synvisc-One, 48 mg for Gel-One, and 60 mg for Durolane (Table 1).
The disparate properties of current HA formulations underlie current efforts to isolate variables meaningful to sustained symptom control. While the same properties may be relevant to joint protection, identifying the most advantageous formulation at an optimal molecular weight and dose has brought HA through several generations. The ability of currently available single injections to provide pain relief for up to six months may be tied to molecular events that trigger relatively durable anti-inflammatory and anti-nociceptive effects.(32,33) Extending these effects present a target for therapies that will improve long-term outcome.
Conclusion
Exogenous HA products have been marketed for the treatment of OA for more than 15 years. Efforts to improve on exogenous HA therapy have generated an array of products with characteristics potentially meaningful to both safety and efficacy. Non-avian derived HA, for example, circumvents risk of allergic reactions, while high molecular weight products are credited with providing longer duration of action. Increasing the dose of HA has the potential for further extending activity and improving binding to CD44, the chondrocyte receptor by which HA may mediate both its viscoelastic properties and its homeostatic effects on joint integrity. The differences between products provide a basis for the experimental and clinical studies that will better define the most important activities of HA in regard to OA therapy.
References
1. Laurent TC, Laurent UB, Fraser JR. The structure and function of hyaluronan: An overview. Immunology and cell biology 1996;74:A1-7.
2. Hunter DJ, Felson DT. Osteoarthritis. Bmj 2006;332:639-42.
3. Kogan G, Soltes L, Stern R, Gemeiner P. Hyaluronic acid: a natural biopolymer with a broad range of biomedical and industrial applications. Biotechnology letters 2007;29:17-25.
4. Han TY, Lee JW, Lee JH , et al. Subdermal minimal surgery with hyaluronic acid as an effective treatment for neck wrinkles. Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al] 2011;37:1291-6.
5. Rydell N, Balazs EA. Effect of intra-articular injection of hyaluronic acid on the clinical symptoms of osteoarthritis and on granulation tissue formation. Clinical orthopaedics and related research 1971;80:25-32.
6. Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G. Viscosupplementation for the treatment of osteoarthritis of the knee. The Cochrane database of systematic reviews 2006:CD005321.
7. Ray TR. Using viscosupplementation to treat knee osteoarthritis. The Physician and sportsmedicine 2013;41:16-24.
8. Dahl LB, Dahl IM, Engstrom-Laurent A, Granath K. Concentration and molecular weight of sodium hyaluronate in synovial fluid from patients with rheumatoid arthritis and other arthropathies. Annals of the rheumatic diseases 1985;44:817-22.
9. Moreland LW. Intra-articular hyaluronan (hyaluronic acid) and hylans for the treatment of osteoarthritis: mechanisms of action. Arthritis research & therapy 2003;5:54-67.
10. Balazs EA. The physical properties of synovial fluid and the spcific role of hyaluronic acid. In: Heifert AJ, ed. Disorders of the Knee. Philadelphia: J.B. Lippincott; 1982:61-74.
11. Yasui T, Akatsuka M, Tobetto K, Hayaishi M, Ando T. The effect of hyaluronan on interleukin-1 alpha-induced prostaglandin E2 production in human osteoarthritic synovial cells. Agents and actions 1992;37:155-6.
12. Pozo MA, Balazs EA, Belmonte C. Reduction of sensory responses to passive movements of inflamed knee joints by hylan, a hyaluronan derivative. Experimental brain research 1997;116:3-9.
13. Grigolo B, Roseti L, Fiorini M, et al. Transplantation of chondrocytes seeded on a hyaluronan derivative (hyaff-11) into cartilage defects in rabbits. Biomaterials 2001;22:2417-24.
14. Park SH, Park SR, Chung SI, Pai KS, Min BH. Tissue-engineered cartilage using fibrin/hyaluronan composite gel and its in vivo implantation. Artificial organs 2005;29:838-45.
15. Nehrer S, Domayer S, Dorotka R, Schatz K, Bindreiter U, Kotz R. Three-year clinical outcome after chondrocyte transplantation using a hyaluronan matrix for cartilage repair. European journal of radiology 2006;57:3-8.
16. Zimmer. Gel-One Prescribing Information. http://www.zimmer. com/content/pdf/en-US/Gel-One_Pkg_Insert_Final.pdf2014.
17. Shimada E, Matsumura G. Viscosity and molecular weight of hyaluronic acids. Journal of biochemistry 1975;78:513-7.
18. Takahashi T, Uemura Y, Taguchi H, et al. Cross talk between COX-2 inhibitor and hyaluronic acid in osteoarthritic chondrocytes. International journal of molecular medicine 2004;14:139-44.
19. Nakamura H, Kenmotsu S, Sakai H, Ozawa H. Localization of CD44, the hyaluronate receptor, on the plasma membrane of osteocytes and osteoclasts in rat tibiae. Cell and tissue research 1995;280:225-33.
20. Sandell LJ, Aigner T. Articular cartilage and changes in arthritis. An introduction: cell biology of osteoarthritis. Arthritis research 2001;3:107-13.
21. Tortorella MD, Malfait AM, Deccico C, Arner E. The role of ADAM-TS4 (aggrecanase-1) and ADAM-TS5 (aggrecanase-2) in a model of cartilage degradation. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 2001;9:539-52.
22. Ishida O, Tanaka Y, Morimoto I, Takigawa M, Eto S. Chondrocytes are regulated by cellular adhesion through CD44 and hyaluronic acid pathway. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research 1997;12:1657-63.
23. Chow G, Nietfeld JJ , Knudson CB, Knudson W. Antisense inhibition of chondrocyte CD44 expression leading to cartilage chondrolysis. Arthritis and rheumatism 1998;41:1411-9.
24. Kawasaki K, Ochi M, Uchio Y, Adachi N, Matsusaki M. Hyaluronic acid enhances proliferation and chondroitin sulfate synthesis in cultured chondrocytes embedded in collagen gels. Journal of cellular physiology 1999;179:142-8.
25. Frean SP, Abraham LA, Lees P. In vitro stimulation of equine articular cartilage proteoglycan synthesis by hyaluronan and carprofen. Research in veterinary science 1999;67:183-90.
26. Takahashi K, Goomer RS, Harwood F, Kubo T, Hirasawa Y, Amiel D. The effects of hyaluronan on matrix metalloproteinase-3 (MMP-3), interleukin-1beta(IL-1beta), and tissue inhibitor of metalloproteinase-1 (TIMP-1) gene expression during the development of osteoarthritis. Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 1999;7:182-90.
27. Grishko V, Xu M, Ho R, et al. Effects of hyaluronic acid on mitochondrial function and mitochondria-driven apoptosis following oxidative stress in human chondrocytes. The Journal of biological chemistry 2009;284:9132-9.
28. Lee YT, Shao HJ , Wang JH , Liu HC, Hou SM, Young TH. Hyaluronic acid modulates gene expression of connective tissue growth factor (CTGF), transforming growth factor-beta1 (TGF-beta1), and vascular endothelial growth factor (VEGF) in human fibroblast-like synovial cells from advanced-stage osteoarthritis in vitro. Journal of orthopaedic research : official publication of the Orthopaedic Research Society 2010;28:492-6.
29. Smith MM, Ghosh P. The synthesis of hyaluronic acid by human synovial fibroblasts is influenced by the nature of the hyaluronate in the extracellular environment. Rheumatology international 1987;7:113-22.
30. Sakakibara Y, Miura T, Iwata H, et al. Effect of high-molecular weight sodium hyaluronate on immobilized rabbit knee. Clinical orthopaedics and related research 1994:282-92.
31. Yoshimi T, Kikuchi T, Obara T, et al. Effects of high-molecular weight sodium hyaluronate on experimental osteoarthrosis induced by the resection of rabbit anterior cruciate ligament. Clinical orthopaedics and related research 1994:296-304.
32. Vitanzo PC, Jr., Sennett BJ. Hyaluronans: is clinical effectiveness dependent on molecular weight? American journal of orthopedics 2006;35:421-8.
33. Kelly MA, Moskowitz RW, Lieberman JR. Hyaluronan therapy: looking toward the future. American journal of orthopedics 2004;33:23-8.
Chapter 2: Hyaluronic Acid in the Knee: History, Characteristics and Efficacy
In the knee, hyaluronic acid (HA), a naturally-occurring compound with viscoelastic properties, is credited with several physiologic functions associated with joint homeostasis. This includes a role in compression force distribution, tissue lubrication, and regulation of cellular activities.(1) In patients with osteoarthritis (OA) of the knee, a chronic degenerative process that adversely affects both cartilage and bone,(2) viscosupplementation with exogenously-produced formulations of HA has been available for more than 15 years. Direct comparisons between current products remain limited, but the distinctions between treatments are potentially important for clinical activity. These distinctions, which may influence onset and duration of pain relief as well as safety, include composition, molecular weight, and molecular activity. Consideration of the physiochemical properties of HA may also be relevant to the more challenging goal of slowing or preventing further joint deterioration.
Show review