Expert Review
Strategies beyond Statins for Control of Dyslipidemias
Chapter 2: Bile Acid Sequestrants: Rediscovering an Alternative to Statins
Robert A. Hegele, MD, FRCPC
Jacob J. Wolfe Distinguished Medical Research Chair
Edith Schulich Vinet Canada Research Chair (Tier 1) in Human Genetics
Martha Blackburn Chair in Cardiovascular Research
Distinguished University Professor of Medicine and Biochemistry
University of Western Ontario
London, Ontario
Bile acid sequestrants have been employed in the treatment of dyslipidemias for nearly 50 years. Over the past two decades, their role has been overshadowed by HMG CoA reductase inhibitors (statins), which produce larger reductions in low density lipoprotein cholesterol (LDL-C) levels and have been more extensively studied in multinational clinical trials. However, bile acid sequestrants can offer substantial reductions in LDL-C making them an appropriate substitute in patients who cannot tolerate statins and an adjunctive therapy in patients who are not reaching treatment goals on statins alone. The lipid lowering mechanism of bile acid sequestrants, which is now understood in detail that was not available when these agents were first shown to reduce cardiovascular events, is complementary and additive to that of statins. Newer formulations of bile acid sequestrants may make this class of drug more convenient and better tolerated.
Mechanism of Action
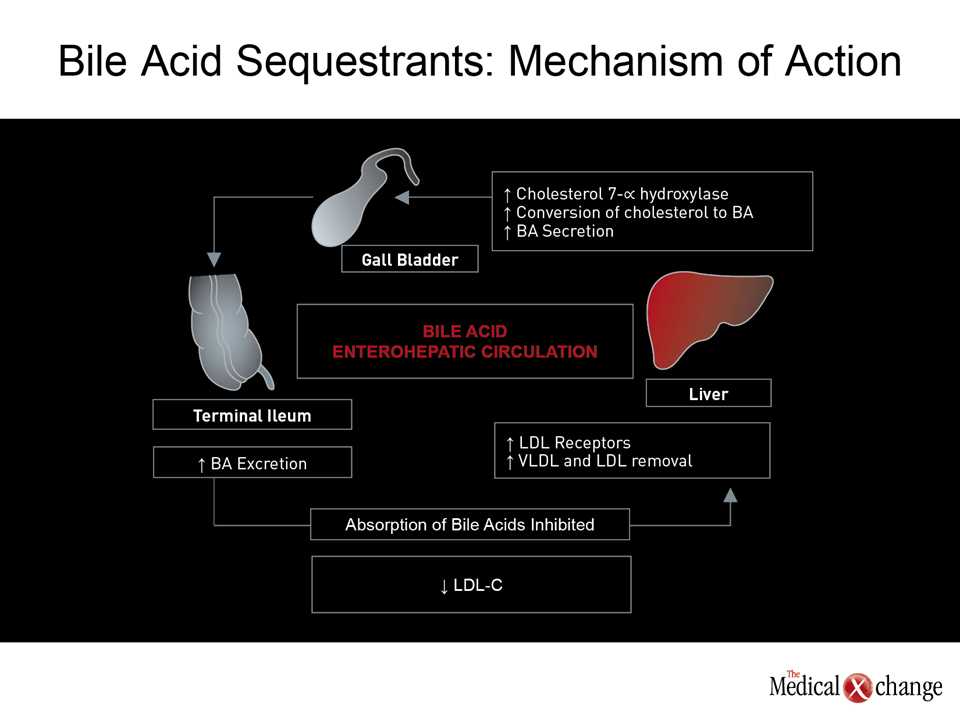
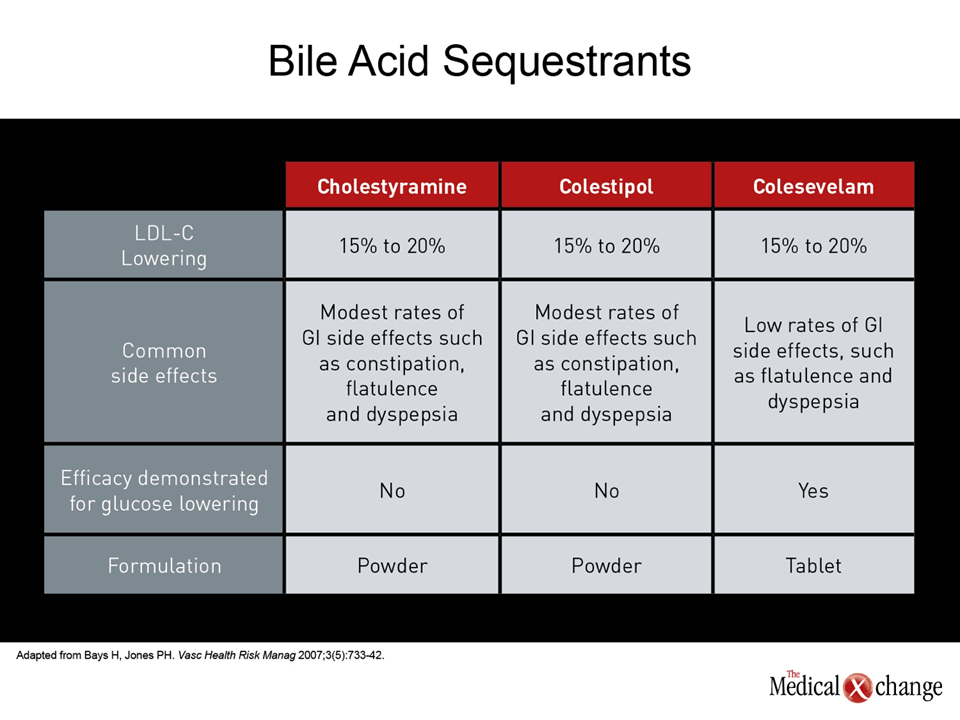
Bile acid sequestrants were the first agents to demonstrate that pharmacologic reductions in LDL-C can reduce cardiovascular (CV) events. In 1964, they were the first pharmacologic agent to receive regulatory approval for this indication. Their mechanism is dependent on the important role played by bile acids in cholesterol homeostasis. Bile acids are released from the gallbladder after a meal into the gastrointestinal tract to aid digestion.(1)Normally, about 95% of bile acids are reabsorbed in the terminal ileum and returned to the liver through the enterohepatic circulation. Replenishment of lost bile acids is performed by hepatocytes, which synthesize bile acids from cholesterol. When bile acid sequestrants inhibit the absorption of bile acids and their return through the enterohepatic circulation, the cholesterol pool in the liver becomes depleted as the liver directs more cholesterol towards synthesis of bile acids to keep up with their loss into the large intestine. As a result, LDL receptor expression on hepatocytes is upregulated to draw cholesterol from the circulation. The upregulation of the LDL receptor is considered the key final common pathway for removing cholesterol from the circulation.(2)This lowers both total cholesterol and LDL-C (Fig. 1). The activity of bile acid sequestrants differs from that of the cholesterol absorption inhibitor ezetimibe, which blocks the Niemann-Pick C1-like (NPC1L1) receptor, a central mediator of cholesterol uptake by enterocytes in the upper small intestine (duodenum and jejunum).(3)As a result, ezetimibe prevents cholesterol absorption at the brush border of the upper small intestine. The final result is depletion of the liver cholesterol pool and upregulation of the LDL receptor in order to increase LDL particle uptake and replenish the cholesterol in the liver. However, in contrast to bile acid sequestrants, ezetimibe is absorbed through the GI tract and is extensively metabolized to an active phenolic glucuronide which reaches the systemic circulation after oral administration.(4)Bile acid sequestrants are not absorbed and their distribution is limited to the GI lumen.(5)However, both classes of intestinal drugs – cholesterol absorption inhibitors and bile acid sequestrants – ultimately upregulate hepatocyte LDL receptors and this results in increased LDL particle uptake and decreased plasma levels of LDL. Once thought to be relatively inert, bile acids also seem to have endocrinologic functions that affect several digestive and metabolic processes.(6)They have a significant role in the regulation of gastrointestinal (GI) motility, they mediate water and electrolyte absorption, and they influence nutrient absorption. More recently, they have been shown to influence glucose metabolism to a sufficient degree that bile acid sequestrants have been extensively evaluated as an adjunctive treatment in type 2 diabetes mellitus (DM2).(7) The mechanism of the beneficial effect on glycemia is not fully understood, but is thought to be mediated through incretins or via incretin-like effects. The three bile acid sequestrants available for clinical use are cholestyramine, colestipol, and colesevelam. The basic mechanisms of these agents for lowering plasma cholesterol are comparable, but there are structural differences that alter bile acid binding activity and side effect profile. Cholestyramine and colestipol are considered first generation agents, while colesevelam, a second-generation agent, has greater bile acid binding affinity and greater potency on a milligram basis than the other two. All of the most common side effects of bile acid sequestrants, including flatulence, dyspepsia, and diarrhea, have been lower on colesevelam than on cholestyramine.(8-9)In particular, colesevelam is not associated with significant constipation.(10)In addition, while first-generation agents impaired uptake of a broad range of drugs, such as propranolol, thiazide diuretics, and penicillin, such drug interactions have not been reported for colesevelam.(11)Not least important, colesevelam, unlike other bile acid sequestrants, which are produced in powder form, is available in a tablet formulation.
Clinical Trials: Efficacy and Safety
Clinical trials have demonstrated benefits of bile acids sequestrants on cardiovascular outcomes, lipid profile, and atherosclerosis as assessed by non-invasive imaging. The more recent evidence of a beneficial effect on glycemic control may have relevance to cardiovascular risk as well as prevention of the complications of diabetes. The earliest major clinical trial to demonstrate primary prevention of major adverse CV events (MACE) was the Lipid Research Clinics Coronary Prevention Trial (LRCCPT), which compared 24 gm per day of cholestyramine to placebo in 3806 men with risk factors for CV disease.(12)The average LDL-C reduction from baseline was 20.3% over the duration of the study. Over a mean duration of 7.4 years, the rate of fatal and non-fatal myocardial infarctions (MIs) among those randomized to the bile acid sequestrant was 19% lower than in the group given placebo. It is notable that this reduction in events was achieved despite relatively poor compliance that reduced the average daily dose to 14 gm per day. A correlation was subsequently shown between amount of drug taken, degree of LDL-C lowering, and risk reduction (Fig. 2). Further with respect to atherosclerotic events, an abstract presented at the 2012 American Diabetes Association (ADA) Scientific Meeting used a national healthcare claims database to link at least 6 months adherence to colesevelam with a significant reduction in CV events among patients with type 2 diabetes (DM2) (Ye et al. ADA 2012 Abs 939-P). Given the limitations of this type of observational study of a database, the results were nonetheless consistent with the reduction of atherosclerotic events seen with cholestyramine in LRC-CPPT. Of course, prospective confirmation of this benefit in a randomized clinical trial is needed. Bile acid sequestrants were also employed in some of the earliest studies that demonstrated an association between reductions in LDL-C and stabilized or even improved atherosclerotic plaque burden on angiography. In the NHLBI Type II Coronary Intervention Study, 119 patients were placed on a low-cholesterol diet and then randomized to 24 mg day of cholestyramine or placebo.(13)At the end of 5 years of treatment, there was a 65% reduction in atherosclerotic plaque progression from baseline in those randomized to the bile acid sequestrants relative to placebo. These studies were followed by a series of angiographic studies that showed an association between LDL-C reduction and altered progression of atherosclerosis. For instance, in the Cholesterol Lowering Atherosclerosis Study (CLAS I),(14)the follow-up CLAS II study,(15)and the Familial Atherosclerosis Treatment Study (FATS),(16)there were consistent reductions in progression and increases in regression of plaques on coronary angiograms in those receiving active therapy compared to those receiving placebo. In CLAS-I, the active therapy was a combination of colestipol and niacin, which reduced LDL-C by approximately 40% and increased HDL-C by more than 35%. In FATS, colestipol was combined with lovastatin to produce a 46% reduction in LDL-C and a 15% increase in HDL-C. Other regression studies with a bile acid sequestrant alone, such as the St. Thomas Atherosclerosis Regression Study (STARS),(17)which employed cholestyramine, also contributed to evidence that LDL-C reductions slow or even reverse atherosclerotic disease. Finally, with respect to glycemic control, several small studies have associated bile acid sequestrants alone or in combination with anti-diabetic agents with favorable effects in patients with type 2 diabetes mellitus (DM2). For instance, in a 6-week, placebo-controlled crossover study with cholestyramine, the bile acid sequestrants was associated with a 13% reduction in fasting glucose and a 0.5% reduction in HbA1c.(18)Similar results were achieved with a pilot study of colesevelam and supported by a subsequent meta-analysis of 8 additional colesevelam studies.(19-20)
Guidelines: Role of Bile Acid Sequestrants
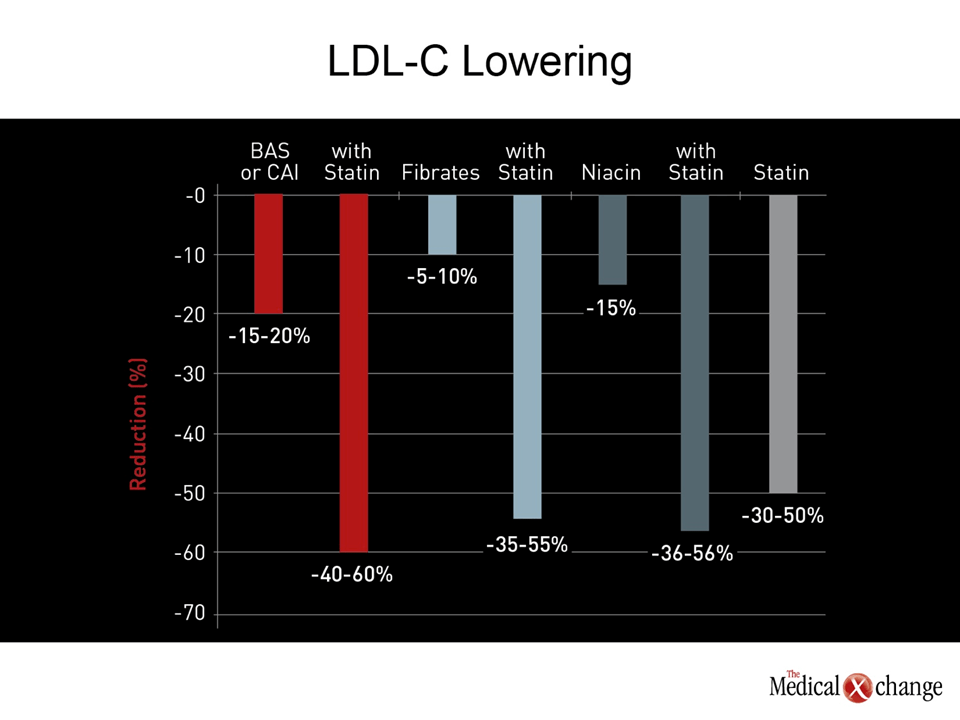
Statins remain the first-line treatment for control of LDL-C in all major guidelines. Numerous studies have confirmed the efficacy of this class of agents in reducing both LDL-C and risk of CV events (Fig. 3). However, adjunctive and alternative agents are often needed to reach current treatment goals and for patients who are unable to tolerate appropriate statin doses. Of those placed on statin monotherapy, approximately one third may not reach treatment goals, especially with increasingly strict recommended target levels of LDL-C.(21)In addition, there is a small but substantial rate of statin intolerance, variably estimated between 5% and 10% in clinical practice.(22) Effective and safe alternatives to statins are needed in this situation as well. In those who require alternative or adjunctive agents beyond diet and other lifestyle changes to reach goals, the choices include bile acid sequestrants, the cholesterol absorption inhibitor ezetimibe, fibrates, and niacin. While more than one of these agents may be appropriate in any specific individual, accompanying cardiovascular risk markers might be one factor to influence the choice of a specific agent. For example, bile acid sequestrants increase triglycerides, suggesting fibrates may be a more appropriate choice in patients with significant hypertriglyceridemia. Niacin, which can induce flushing even with controlled release formulations, is widely considered appropriate for patients with depressed HDL-C levels. However, the Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides (AIM-HIGH) study was unable to show a reduction in CV events despite a median 20% increase in HDL-C and a median 16% reduction in LDL-C,(23)introducing controversy about the role of extended release niacin in CV risk reduction in patients already on statin therapy. Bile acid sequestrants and ezetimibe offer the specific reductions in LDL-C. Event reductions proven with bile acid sequestrants as monotherapy have never been shown with ezetimibe as monotherapy. Both bile acid sequestrants and ezetimibe, however, offer complementary and additive LDL-C reduction when combined with a statin and can help patients reach their LDL-C targets. Due to their favorable effect on glucose metabolism, bile acid sequestrants may be particularly attractive in patients with DM2 when triglyceride control is not problematic.
Compliance and Bile Acid Sequestrants
Since the time they were introduced, statins were seen as a substitute for bile acid sequestrants not only because they offered more potent lipid lowering but because they were better tolerated. However, the side effects associated with bile acid sequestrants are typically mild, while the benefits from reducing LDL-C to target are potentially substantial in patients who are not at target or who are intolerant to statins. Considering strategies that will induce patients to remain compliant with these agents is of course critical to the delivery of their clinical benefits (Fig. 4). While GI complaints are generally the most prominent adverse events with all bile acid sequestrants, the greater relative tolerability of the second-generation agent colesevelam has been associated with high rates of compliance, reaching 93% in one study, which was comparable to the rate of compliance seen with placebo.(9)The availability of colesevelam as a tablet is also convenient for dosing. Both features may influence the decision in selecting a bile acid sequestrant to combine with other therapies, including statins, because of the critical role of long-term adherence in deriving benefits.
Conclusion
The clinical value of bile acid sequestrants in achieving LDL-C goals in selected patients should not be overlooked. Although the linear relationship between reductions in LDL-C and the protection from CV events was primarily demonstrated with statins, guidelines suggest that the LDL-C target can be attained with other agents when statin monotherapy is insufficient. Due to the stringent target LDL-C levels specified in recent lipid guidelines, adjunctive therapies are increasingly required. As an adjunctive or alternative therapy, bile acid sequestrants can be useful for helping patients at risk attain these LDL-C targets. Their lipid lowering effect is complementary to that provided by statins. By increasing the proportion of patients who attain LDL-C targets, bile acid sequestrants have the potential to further reduce the risk of preventable CV events.
References
1. Staels B, Fonseca VA. Bile acids and metabolic regulation: mechanisms and clinical responses to bile acid sequestration. Diabetes Care 2009;32 Suppl 2:S237-45. 2. Llorente-Cortes V, Otero-Vinas M, Sanchez S, Rodriguez C, Badimon L. Low-density lipoprotein upregulates low-density lipoprotein receptor-related protein expression in vascular smooth muscle cells: possible involvement of sterol regulatory element binding protein-2-dependent mechanism. Circulation 2002;106(24):3104-10. 3. Garcia-Calvo M, Lisnock J, Bull HG, et al. The target of ezetimibe is Niemann-Pick C1-Like 1 (NPC1L1). Proc Natl Acad Sci U S A 2005;102(23):8132-7. 4. Ghosal A, Hapangama N, Yuan Y, et al. Identification of human UDP-glucuronosyltransferase enzyme(s) responsible for the glucuronidation of ezetimibe (Zetia). Drug Metab Dispos 2004;32(3):314-20. 5. Bays H, Dujovne C. Colesevelam HCl: a non-systemic lipid-altering drug. Expert Opin Pharmacother 2003;4(5):779-90. 6. Houten SM, Watanabe M, Auwerx J. Endocrine functions of bile acids. EMBO J 2006;25(7):1419-25. 7. Goldberg RB, Rosenson RS, Hernandez-Triana E, Misir S, Jones MR. Initial combination therapy with metformin plus colesevelam improves lipoprotein particles in patients with early type 2 diabetes mellitus. J Clin Lipidol 2012;6(4):318-24. 8. Aldridge MA, Ito MK. Colesevelam hydrochloride: a novel bile acid-binding resin. Ann Pharmacother 2001;35(7-8):898-907. 9. Steinmetz KL. Colesevelam hydrochloride. Am J Health Syst Pharm 2002;59(10):932-9. 10. Davidson MH, Dillon MA, Gordon B, et al. Colesevelam hydrochloride (cholestagel): a new, potent bile acid sequestrant associated with a low incidence of gastrointestinal side effects. Arch Intern Med 1999;159(16):1893-900. 11. Bays H, Jones PH. Colesevelam hydrochloride: reducing atherosclerotic coronary heart disease risk factors. Vasc Health Risk Manag 2007;3(5):733-42. 12. The Lipid Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of coronary heart disease. JAMA 1984;251(3):351-64. 13. Brensike JF, Levy RI, Kelsey SF, et al. Effects of therapy with cholestyramine on progression of coronary arteriosclerosis: results of the NHLBI Type II Coronary Intervention Study. Circulation 1984;69(2):313-24. 14. Blankenhorn DH, Nessim SA, Johnson RL, Sanmarco ME, Azen SP, Cashin-Hemphill L. Beneficial effects of combined colestipol-niacin therapy on coronary atherosclerosis and coronary venous bypass grafts. JAMA 1987;257(23):3233-40. 15. Cashin-Hemphill L, Mack WJ, Pogoda JM, Sanmarco ME, Azen SP, Blankenhorn DH. Beneficial effects of colestipol-niacin on coronary atherosclerosis. A 4-year follow-up. JAMA 1990;264(23):3013-7. 16. Brown G, Albers JJ, Fisher LD, et al. Regression of coronary artery disease as a result of intensive lipid-lowering therapy in men with high levels of apolipoprotein B. N Engl J Med 1990;323(19):1289-98. 17. Watts GF, Lewis B, Brunt JN, et al. Effects on coronary artery disease of lipid-lowering diet, or diet plus cholestyramine, in the St Thomas’ Atherosclerosis Regression Study (STARS). Lancet 1992;339(8793):563-9. 18. Garg A, Grundy SM. Cholestyramine therapy for dyslipidemia in non-insulin-dependent diabetes mellitus. A short-term, double-blind, crossover trial. Ann Intern Med 1994;121(6):416-22. 19. Zieve FJ, Kalin MF, Schwartz SL, Jones MR, Bailey WL. Results of the glucose-lowering effect of WelChol study (GLOWS): a randomized, double-blind, placebo-controlled pilot study evaluating the effect of colesevelam hydrochloride on glycemic control in subjects with type 2 diabetes. Clin Ther 2007;29(1):74-83. 20. Aggarwal S, Loomba RS, Arora RR. Efficacy of colesevelam on lowering glycemia and lipids. J Cardiovasc Pharmacol 2012;59(2):198-205. 21. Waters DD, Brotons C, Chiang CW, et al. Lipid treatment assessment project 2: a multinational survey to evaluate the proportion of patients achieving low-density lipoprotein cholesterol goals. Circulation 2009;120(1):28-34. 22. Eckel RH. Approach to the patient who is intolerant of statin therapy. J Clin Endocrinol Metab 2010;95(5):2015-22. 23. Boden WE, Probstfield JL, Anderson T, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011;365(24):2255-67.
Chapter 2: Bile Acid Sequestrants: Rediscovering an Alternative to Statins
Bile acid sequestrants have been employed in the treatment of dyslipidemias for nearly 50 years. Over the past two decades, their role has been overshadowed by HMG CoA reductase inhibitors (statins), which produce larger reductions in low density lipoprotein cholesterol (LDL-C) levels and have been more extensively studied in multinational clinical trials. However, bile acid sequestrants can offer substantial reductions in LDL-C making them an appropriate substitute in patients who cannot tolerate statins and an adjunctive therapy in patients who are not reaching treatment goals on statins alone. The lipid lowering mechanism of bile acid sequestrants, which is now understood in detail that was not available when these agents were first shown to reduce cardiovascular events, is complementary and additive to that of statins. Newer formulations of bile acid sequestrants may make this class of drug more convenient and better tolerated.
Show review