Expert Review
Strategies beyond Statins for Control of Dyslipidemias
Chapter 3: Dyslipidemia in Patients with Type 2 Diabetes: Special Challenges
Vincent Woo, MD, FRCPC
University of Manitoba, Winnipeg, Manitoba
Cardiovascular (CV) disease accounts for a large proportion of the excess and premature mortality related to type 2 diabetes mellitus (DM2). In relation to age-matched individuals, people with DM2 are two to three times more likely to have a CV event than age-matched people without diabetes.(1) According to data from the Canadian Diabetes Association (CDA), approximately 80% of patients with DM2 die of CV disease or stroke, which is a rate that is 2 to 4 times greater than in patients without diabetes.(2) Optimal protection from CV events depends on tight control of the major risk factors that are commonly identified in patients with DM2, including hyperlipidemia and hypertension in addition to hyperglycemia.
Of these risk factors, hyperlipidemia deserves particular attention. Data from several studies, including UKPDS, support the premise that tight control of lipids, relative to tight control of other risk factors, provides the greatest relative protection against CV events.(3) In the STENO-2 trial, there was a 57% relative reduction in CV events observed among those reaching treatment goals for lipids, blood pressure, and blood glucose relative to those who did not,(4)but the authors reported that reaching lipid targets may have provided the greatest relative contribution to risk reduction.
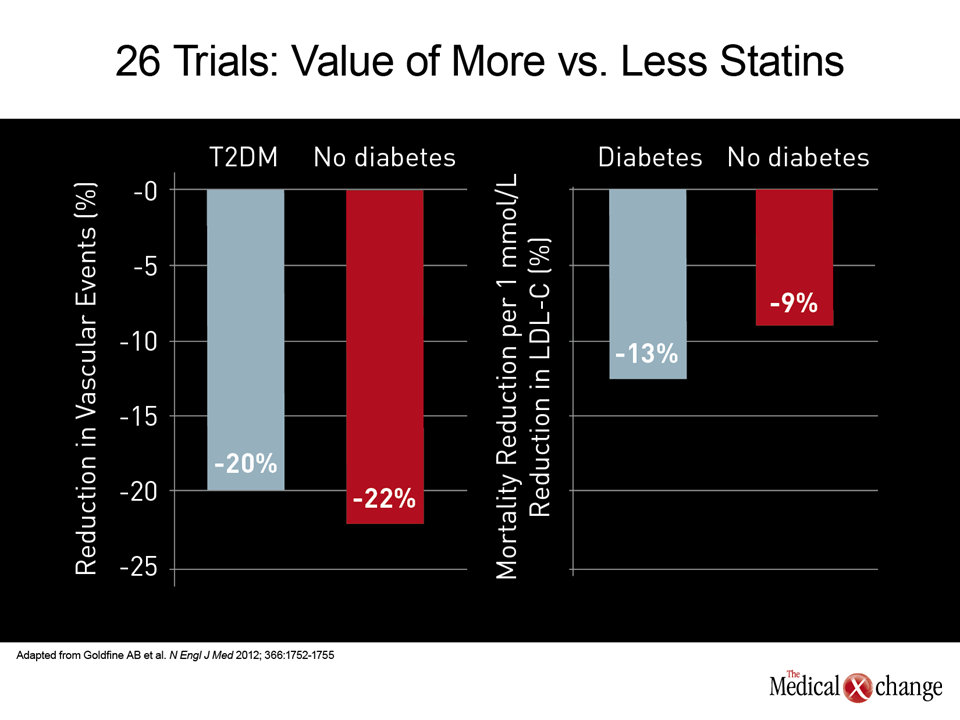
HMG-CoA reductase inhibitors (statins) are the first-line pharmacologic therapy for reaching guideline recommended goals for low density lipoprotein cholesterol (LDL-C). In the large statin trials that included DM2 patients, post-hoc analyses suggest that the highly favorable risk-to-benefit ratio, including an all-cause mortality benefit, has been at least as large in those with DM2 as those without (Fig. 1).(5) In many major guidelines, including those newly issued by the Canadian Cardiovascular Society,(6), the presence of DM2 is considered an indication for seeking the most aggressive LDL-C goals. Perhaps due to the difficulty of reaching these low levels, the proportion of patients with DM2 at target is low.(7-8) Strategies to increase the proportion of DM2 patients at treatment goals have major implications for risk reductions. Statins are effective and generally well tolerated, but it is important to recognize that these agents are not the only pharmacologic tool for lipid lowering, particularly when confronted with patients with DM2 who cannot reach treatment goals on statins alone. While other lipid lowering agents, such as bile acid sequestrants, lipid absorption inhibitors, and fibrates are typically employed in the small proportion of patients who are intolerant to statins, it is important to consider adjunctive use of these agents in those who cannot reach treatment goals on statins alone or at a dose of statin that is acceptably tolerated. The frequency with which patients with DM2 remain above treatment goals represents a large missed opportunity to reduce the rate of CV events.
Epidemiology of Lipid Abnormalities in Type 2 Diabetes
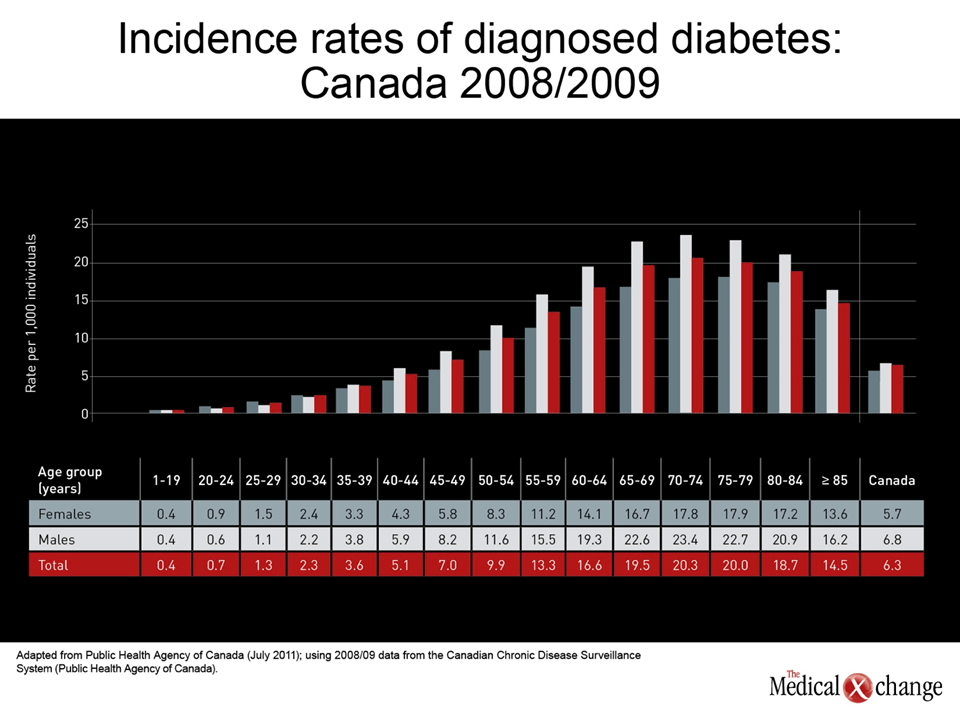
The prevalence of diabetes is on a steep upwards trajectory. Between 2010 and 2030, there will be an estimated 70% increase in the number of adults with diabetes in developing countries and a 20% increase in developed countries(9). The age- and sex-adjusted diabetes prevalence in Canada will increase by 40%, from 6.8% in 2010 to 9.9%, or 3.4 million in 2020! A majority of these people have type 2 diabetes and many of whom have dyslipidemia, which is characterized by elevated plasma triglyceride levels, low levels of high-density lipoprotein cholesterol (HDL-C), and small, dense atherogenic low-density lipoprotein (LDL) particles. Although statins are efficacious in patients with type 2 diabetes, rates of cardiovascular events remain elevated in such patients even after statin treatment. Diabetes has turned into an epidemic in industrialized countries driven by the increasing rates of obesity.(10)In Canada, like the United States,(11) there has been a corresponding rise in the rates of obesity and diabetes over the past several decades.(12) The Canadian Diabetes Association (CDA) estimates that 9 million Canadians, or about 25% of the population, now have diabetes or meet the current definition of prediabetes (Fig. 2). (2) Of those with diabetes, approximately 90% have DM2. Further growth in the proportion of the population that is obese and that have diabetes is predicted.(13) This has enormous public health implications. In particular, these trends predict a corresponding rise in cases of myocardial infarction (MI), stroke, congestive heart disease, and other consequences of vascular dysfunction, which are closely correlated with both obesity and DM2.(14) Patients with DM2 typically have multiple risk factors for CV disease, including dyslipidemia and hypertension. A comprehensive approach to CV risk management is therefore appropriate in this population, but dyslipidemias deserve emphasis. Some of the most compelling evidence of CV and stroke risk reduction from intervention directed at a modifiable risk factor has been generated by lipid lowering studies. The relative benefit has largely been derived from ad hoc analyses of DM2 patients who participated in the major statin trials, but consistency of benefit across trials supports current treatment recommendations, including those from the Canadian Cardiovascular Society (CCS).(15)
Dyslipidemia in Diabetes
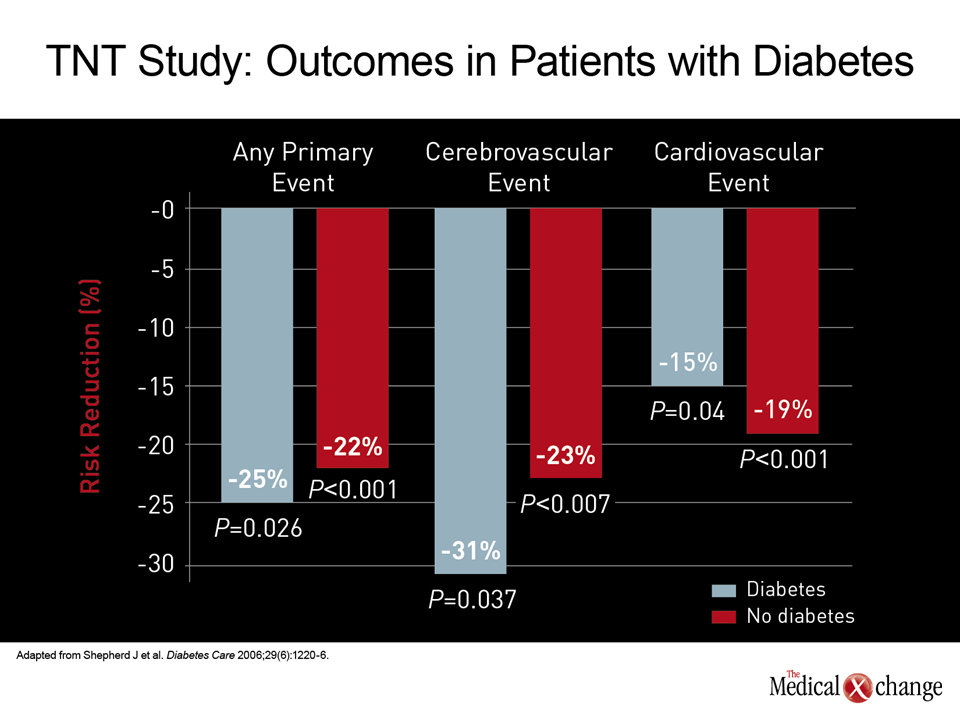
Despite the fact that reaching guideline-recommended LDL-C targets should be considered a priority for CV risk reduction, patients with DM2 do not have higher average LDL-C levels than those without diabetes.(16) However, there is evidence that LDL-C associated with DM2 has greater atherogenicity due to smaller and denser LDL-C particles.(17) It is notable that hypertriglyceridemia and low HDL-C are far more characteristic of the dyslipidemias associated with DM2, but the value of treating these lipid abnormalities is far less well established than lowering LDL-C. This is not to discount the value of reducing elevated triglycerides, which may contribute to the atherogenicity of LDL-C particles, (18) or raising high density lipoprotein cholesterol (HDL-C), which tend to be inversely related to plasma triglyceride levels, (19) but LDL-C targets are a priority because of the robust evidence that this leads to CV event reductions. The benefits of lowering LDL-C in patients with DM2 despite baseline levels that would not necessarily warrant therapy in someone without CV risk factors can be derived from large, multinational studies that included diabetics as well as smaller trials limited to patients with diabetes.(20-21) In the Treating to New Targets (TNT) study for example, the relative benefit of more aggressive lipid lowering in the 1,501 DM2 patients was essentially the same as that in the 8,500 patients without DM2 (Fig. 3). (22) The CV benefits of reducing HDL-C or hypertriglyceridemia in patients with DM2 have been more difficult to show because of the absence of medications that induce a degree of change in these lipid subfractions that is commensurate with the reduction in LDL-C achieved with statins. However, support for considering strategies to lower triglycerides and raise HDL-C can be derived from the strong inverse relationship between HDL-C levels and CV events has been observed in epidemiologic studies.(23) Some mechanistic properties of HDL-C, including a favorable effect on skeletal uptake of glucose, have also been cited among reasons to predict favorable effects from treating this risk factor in patients with DM2.(19) Similarly, the considerable epidemiologic data that link hypertriglyceridemia to CV risk factor (24) have also suggested this lipid abnormality should be addressed along with LDL-C.(25)
Health Behavior and Diet
The best first-line strategy to reduce the threat of DM2 and the risk this disease poses for CV events is to prevent obesity, which is a major source of the increasing rates of DM2 in Canada and elsewhere.(26) Controlled trials have demonstrated that lifestyle changes, particularly weight loss, can prevent or delay the onset of DM2.(26) However, the relatively modest changes over sustained follow-up underline the difficulty of achieving sustained lifestyle changes in many individuals.(27) The potential for weight loss to reverse DM2 has been best demonstrated with a series of studies evaluating the effect of bariatric surgery on this outcome.(28) While many patients with DM2 will not be able to achieve the lifestyle changes required to reverse their disease or to reduce lipids and other treatable risk factors to goals, weight loss, increased exercise, and healthier diets should remain a fundamental part of a therapeutic strategy even if pharmacologic agents are required. Such changes may reduce the need for drug therapies and will have broad health benefits, including indirect effects on vascular health from modification of related but independent pathologic processes, such as hypertension.(29)
Lipid Lowering Goals in Diabetics
Lipid lowering goals for diabetes have been issued by several organizations, including the Canadian Cardiovascular Society (CCS) and the Canadian Diabetes Association (CDA),(15, 30) as well as professional organizations in the United States and Europe.(31-32) The recommendations vary only modestly. In the 2009 CCS guidelines, diabetes places men over the age of 45 years and women over the age of 50 years in the high risk category. Younger patients with diabetes reach the high risk category with additional risk factors. In high risk patients, the LDL-C target is <2 mmol/L or a 50% reduction from the baseline level. Other abnormal lipid subfractions were identified as secondary targets. For HDL-C, the goal was placed in the context of total cholesterol (TC) with a target of a TC/HDL-C ratio of <4.0. The CDA also identifies LDL-C as the primary target but the 2008 CDA guidelines specifically recommend measuring and monitoring HDL-C, triglycerides, and total cholesterol. Like the CCS, the CDA recommends a TC/HDL-C ratio of <4.0, but further recommends treatment if the triglyceride (TG) level exceeds 10.0 mmol/L. Measuring plasma ApoB is identified as optional, but the CDA sets a target for ApoB of 0.9 g/L. Both the CCS and the CDA recommend that statins be combined with other lipid lowering agents when statins alone are not adequate to reach targets. The lipid lowering therapy categories other than statins listed by the CCS are bile acid sequestrants, fibrates, and niacin.
The Need to Treat Beyond Statins
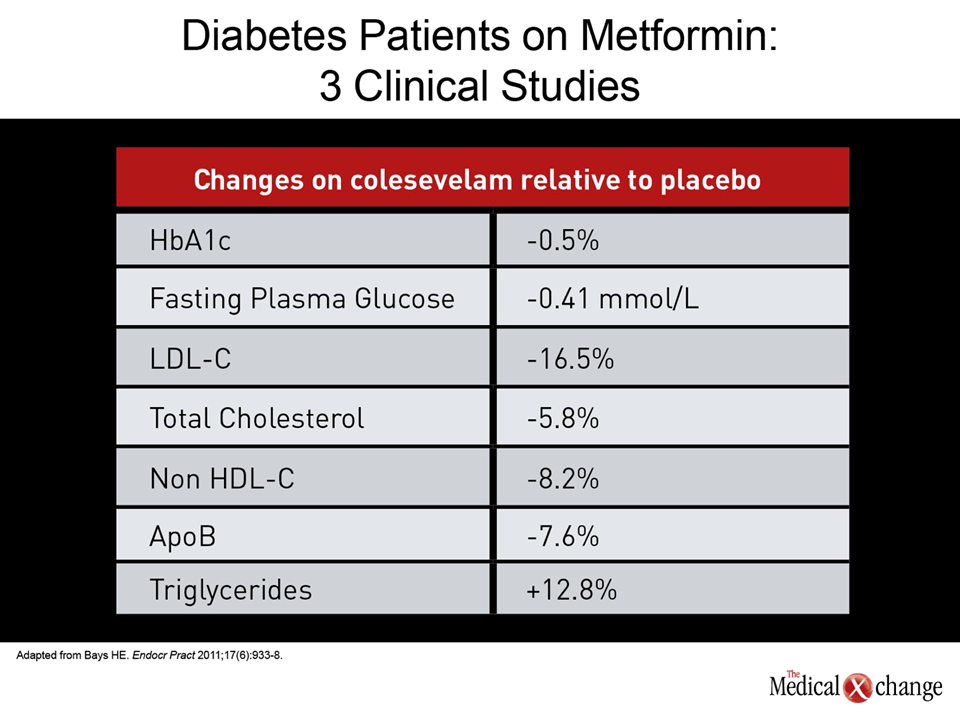
The benefit from statins in DM2 are largely attributable to their ability to lower LDL-C, which have repeatedly been associated with reductions in CV events and stroke in patients with DM2 whether administered for primary or secondary prevention.(33-35) However, a large proportion of patients will require additional lipid lowering agents to achieve LDL-C levels <2.0 mmol/L or a 50% reduction in LDL-C from baseline. In one representative survey evaluation of almost 10,000 patients in 9 countries, only about two-thirds of high risk patients, including those with DM2, were at their LDL-C goal.(36) In lipid management in DM2, adding a second agent has the potential not only to increase the proportion of patients at the LDL-C goal but may, in some cases, correct other dyslipidemias that are less well addressed with statins alone. There is also some evidence that specific lipid lowering agents may modestly improve glucose metabolism, a potentially synergistic effect in risk reduction. In addition, combination strategies have the potential to allow lower doses of statins, thereby reducing the risk of side effects, such as myopathy or hepatotoxicity. The 2009 CCS guidelines, like other major guidelines, list bile acid sequestrants, cholesterol absorption inhibitors, fibrates, and niacin as alternative or adjunctive lipid lowering agents. Of these, niacin has been particularly helpful in raising HDL, although efforts to link this activity with a reduction in cardiovascular events have so far failed,(37) and the characteristic flushing associated with this agent, although reduced with extended-release formulations, can be poorly tolerated.(38)Fibrates have been particularly effective for lowering triglycerides, and gemfibrozil specifically was associated with a reduction in CV events in the Helsinki Heart Study.(39) However, gemfibrozil is not recommended as an adjunct to statins in the 2009 CCS guidelines because of an increased risk of rhabdomyolysis.(15) For reducing LDL-C, which deserves the highest priority for preventing CV events in patients with DM2, as well as others with established CV risk, bile acid sequestrants and cholesterol absorption inhibitors are the most attractive adjunctive to statins. Although these agents, particularly bile acid sequestrants, offer little benefit against elevated triglycerides, and only modest benefit against depressed HDL-C, they can provide up to 20% further reduction in LDL-C when added to a statin.(40) While the only currently available cholesterol absorption inhibitor, ezetimibe, has never been associated with a significant reduction in CV events in a randomized trial when used as monotherapy (SHARP was positive), bile acid sequestrants were the first agent of any kind to associate lipid lowering with a CV event reduction.(41) Although this study was not conducted in patients with DM2, the mechanism of benefit, which is lowering of LDL-C, would be expected to be applicable to all groups at elevated CV risk. While the bile acid sequestrants cholestyramine and colestipol are associated with substantial GI side effects, the newer agent in this category, colesevelam, has largely replaced these first-generation agents because it is more potent and better tolerated,(42-44) More importantly from the point of view of risk management in DM2, colesevelam has been associated with favorable effects on glucose metabolism. (45) In a pooled analysis of three placebo-controlled trials, colesevelam was associated with a 16.5% reduction in LDL (P<0.001), a 7.4% reduction in ApoB (P<0.001), a 0.5% reduction in HbA1c (P<0.001), and a 10% reduction in fasting glucose (P<0.001) (Table 1).(46) This effect on glucose has led to the conclusion that colesevelam, which is now available in a tablet that circumvents the problems of taste and preparation of the powdered formulation,(47) suggests it may be a particularly attractive add-on lipid lowering agent in diabetic patients who are not at treatment goals on statins alone.(48)
Summary
Most people with diabetes are at high risk for cardiovascular disease and multifactorial interventions are necessary for vascular protection and/or reduction of cardiovascular disease risk and events. Statins are first line drug therapy to lower LDL-C and adjunctive therapy may often be required to achieve target lipid values. Both cholesterol absorption inhibitors and bile acid sequestrants are effective second line agents to lower LDL-C. The diagnosis of DM2 confers a high risk of CV events. The benefit of lipid lowering in reducing the risk of CV events, including CV-related mortality, is well established in this population. Numerous studies demonstrate that the rigorous LDL-C goals are difficult to reach on statins alone in high risk populations. Adjunctive agents can increase the proportion of patients at goal while some add-on agents may be useful in addressing other dyslipidemias associated with increased CV risk. Both cholesterol absorption inhibitors and bile acid sequestrants are valuable in helping DM2 patients reach rigorous treatment goals, but the evidence that bile acid sequestrants can favorably affect glucose metabolism make them attractive in this setting. However, all pharmacologic treatments should be added on top of lifestyle changes to address the many concomitant risk factors typically present in DM2 patients, including obesity and hypertension.
References
1. Almdal T, Scharling H, Jensen JS, Vestergaard H. The independent effect of type 2 diabetes mellitus on ischemic heart disease, stroke, and death: a population-based study of 13,000 men and women with 20 years of follow-up. Arch Intern Med 2004;164(13):1422-6. 2. The Prevalence and Costs of Diabetes. 2012. (Accessed July 24, 2012, at http://www.diabetes.ca/diabetes-and-you/what/prevalence/.) 3. Turner RC, Millns H, Neil HA, et al. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23). BMJ 1998;316(7134):823-8. 4. Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358(6):580-91. 5. Goldfine AB. Statins: is it really time to reassess benefits and risks? N Engl J Med 2012;366(19):1752-5. 6. Anderson TJ, Grégoire J, Hegele RA et al. 2012 update of the Canadian Cardiovascular Society guidelines for the diagnosis and treatment of dyslipidemia for the prevention of cardiovascular disease in the adult. Can J Cardiol 2013;29(2):151-67. 7. McFarlane SI, Jacober SJ, Winer N, et al. Control of cardiovascular risk factors in patients with diabetes and hypertension at urban academic medical centers. Diabetes Care 2002;25(4):718-23. 8. Beaton SJ, Nag SS, Gunter MJ, Gleeson JM, Sajjan SS, Alexander CM. Adequacy of glycemic, lipid, and blood pressure management for patients with diabetes in a managed care setting. Diabetes Care 2004;27(3):694-8. 9. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87(1):4-14. 10. Walls HL, Backholer K, Proietto J, McNeil JJ. Obesity and trends in life expectancy. J Obes 2012;2012:107989. 11. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010;303(3):235-41. 12. The Obesity Epidemic in Canada. 2005. (Accessed July 25, 2012, at http://www.parl.gc.ca/Content/LOP/ResearchPublications/prb0511-e.htm.) 13. Lee DS, Chiu M, Manuel DG, et al. Trends in risk factors for cardiovascular disease in Canada: temporal, socio-demographic and geographic factors. CMAJ 2009;181(3-4):E55-66. 14. Poirier P, Giles TD, Bray GA, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006;113(6):898-918. 15. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult – 2009 recommendations. Can J Cardiol 2009;25(10):567-79. 16. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106(25):3143-421. 17. Mooradian AD. Dyslipidemia in type 2 diabetes mellitus. Nat Clin Pract Endocrinol Metab 2009;5(3):150-9. 18. Julius U. Influence of plasma free fatty acids on lipoprotein synthesis and diabetic dyslipidemia. Exp Clin Endocrinol Diabetes 2003;111(5):246-50. 19. Barter PJ. The causes and consequences of low levels of high density lipoproteins in patients with diabetes. Diabetes Metab J 2011;35(2):101-6. 20. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366(9493):1267-78. 21. Wolffenbuttel BH, Franken AA, Vincent HH. Cholesterol-lowering effects of rosuvastatin compared with atorvastatin in patients with type 2 diabetes — CORALL study. J Intern Med 2005;257(6):531-9. 22. Shepherd J, Barter P, Carmena R, et al. Effect of lowering LDL cholesterol substantially below currently recommended levels in patients with coronary heart disease and diabetes: the Treating to New Targets (TNT) study. Diabetes Care 2006;29(6):1220-6. 23. Gordon DJ, Probstfield JL, Garrison RJ, et al. High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation 1989;79(1):8-15. 24. Austin MA, Hokanson JE, Edwards KL. Hypertriglyceridemia as a cardiovascular risk factor. Am J Cardiol 1998;81(4A):7B-12B. 25. Haffner SM. Management of dyslipidemia in adults with diabetes. Diabetes Care 1998;21(1):160-78. 26. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346(6):393-403. 27. Vermunt PW, Milder IE, Wielaard F, et al. A lifestyle intervention to reduce Type 2 diabetes risk in Dutch primary care: 2.5-year results of a randomized controlled trial. Diabet Med 2012;29(8):e223-e31. 28. Shimizu H, Timratana P, Schauer PR, Rogula T. Review of Metabolic Surgery for Type 2 Diabetes in Patients with a BMI < 35 kg/m(2). J Obes 2012;2012:147256. 29. Iestra JA, Kromhout D, van der Schouw YT, Grobbee DE, Boshuizen HC, van Staveren WA. Effect size estimates of lifestyle and dietary changes on all-cause mortality in coronary artery disease patients: a systematic review. Circulation 2005;112(6):924-34. 30. Canadian Diabetes Association 2008 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. 2008. (Accessed July 27, 2012, at www.diabetes.ca.) 31. Haffner SM. Dyslipidemia management in adults with diabetes. Diabetes Care 2004;27 Suppl 1:S68-71. 32. Reiner Z, Catapano AL, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J 2011;32(14):1769-818. 33. Tonelli M, Lloyd A, Clement F, et al. Efficacy of statins for primary prevention in people at low cardiovascular risk: a meta-analysis. CMAJ 2011;183(16):E1189-202. 34. Ward S, Lloyd Jones M, Pandor A, et al. A systematic review and economic evaluation of statins for the prevention of coronary events. Health Technol Assess 2007;11(14):1-160, iii-iv. 35. Kearney PM, Blackwell L, Collins R, et al. Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet 2008;371(9607):117-25. 36. Waters DD, Brotons C, Chiang CW, et al. Lipid treatment assessment project 2: a multinational survey to evaluate the proportion of patients achieving low-density lipoprotein cholesterol goals. Circulation 2009;120(1):28-34. 37. Boden WE, Probstfield JL, Anderson T, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011;365(24):2255-67. 38. Kamanna VS, Ganji SH, Kashyap ML. The mechanism and mitigation of niacin-induced flushing. Int J Clin Pract 2009;63(9):1369-77. 39. Frick MH, Elo O, Haapa K, et al. Helsinki Heart Study: primary-prevention trial with gemfibrozil in middle-aged men with dyslipidemia. Safety of treatment, changes in risk factors, and incidence of coronary heart disease. N Engl J Med 1987;317(20):1237-45. 40. Shanes JG. A review of the rationale for additional therapeutic interventions to attain lower LDL-C when statin therapy is not enough. Curr Atheroscler Rep 2012;14(1):33-40. 41. The Lipid Research Clinics Coronary Primary Prevention Trial results. I. Reduction in incidence of coronary heart disease. JAMA 1984;251(3):351-64. 42. Aldridge MA, Ito MK. Colesevelam hydrochloride: a novel bile acid-binding resin. Ann Pharmacother 2001;35(7-8):898-907. 43. Puleston J, Morgan H, Andreyev J. New treatment for bile salt malabsorption. Gut 2005;54(3):441-2. 44. Bays H, Dujovne C. Colesevelam HCl: a non-systemic lipid-altering drug. Expert Opin Pharmacother 2003;4(5):779-90. 45. Goldberg RB, Rosenson RS, Hernandez-Triana E, Misir S, Jones MR. Initial combination therapy with metformin plus colesevelam improves lipoprotein particles in patients with early type 2 diabetes mellitus. J Clin Lipidol 2012;6(4):318-24. 46. Bays HE. Colesevelam hydrochloride added to background metformin therapy in patients with type 2 diabetes mellitus: a pooled analysis from 3 clinical studies. Endocr Pract 2011;17(6):933-8. 47. Steinmetz KL. Colesevelam hydrochloride. Am J Health Syst Pharm 2002;59(10):932-9. 48. Rosenstock J, Fonseca VA, Garvey WT, et al. Initial combination therapy with metformin and colesevelam for achievement of glycemic and lipid goals in early type 2 diabetes. Endocr Pract 2010;16(4):629-40.
Chapter 3: Dyslipidemia in Patients with Type 2 Diabetes: Special Challenges
Cardiovascular (CV) disease accounts for a large proportion of the excess and premature mortality related to type 2 diabetes mellitus (DM2). In relation to age-matched individuals, people with DM2 are two to three times more likely to have a CV event than age-matched people without diabetes.(1) According to data from the Canadian Diabetes Association (CDA), approximately 80% of patients with DM2 die of CV disease or stroke, which is a rate that is 2 to 4 times greater than in patients without diabetes.(2) Optimal protection from CV events depends on tight control of the major risk factors that are commonly identified in patients with DM2, including hyperlipidemia and hypertension in addition to hyperglycemia.
Of these risk factors, hyperlipidemia deserves particular attention. Data from several studies, including UKPDS, support the premise that tight control of lipids, relative to tight control of other risk factors, provides the greatest relative protection against CV events.(3) In the STENO-2 trial, there was a 57% relative reduction in CV events observed among those reaching treatment goals for lipids, blood pressure, and blood glucose relative to those who did not,(4)but the authors reported that reaching lipid targets may have provided the greatest relative contribution to risk reduction.
Show review